

- Home
- Companies
- Epinex Diagnostics Inc
- Articles
- Association between Diabetes Mellitus ...
Association between Diabetes Mellitus and chronic kidney disease with Muscle loss and weight loss
Muscle loss / muscle wasting is the condition in which, proteolytic systems for protein degradation are activated, while protein synthesis decreases, thereby resulting in muscle fiber shrinkage. This condition may be due age or might be due some chronic conditions like Diabetes mellitus (DM) or chronic kidney disease (CKD). Extreme muscle wasting often results in weight loss. Such a condition is generally referred to as cachexia, which is a complex metabolic syndrome that is associated with an underlying disease and characterized by muscle loss with or without fat mass loss. In advanced stages of chronic diseases, frequency of cachexia is high. There are inadequate studies with simultaneous evaluation of a long-term change in muscle mass with presence or absence of DM and CKD.

A recent article published in AGING, enrolled 6247 middle-aged adults from the Korean Genome and Epidemiology Study (KoGES). The subjects were followed-up for 16 years and the retention rate was 70.6% at the end of the seventh follow-up phase (16 years of follow-up). Patients were classified into four groups according to the presence or absence of DM and CKD. The primary outcome was muscle depletion and the secondary outcomes included the manifestation of cachexia, all-cause mortality, and the slopes of changes in fat-free mass and weight.
It was observed that muscle depletion was significantly higher in subjects with DM alone and in those with CKD alone than in those without the two conditions; the incidence in subjects with both DM and CKD was the highest. After sequential adjustment for confounding factors, the study found that the risk of muscle depletion development was significantly higher in subjects with DM alone than in those without DM and CKD. Further results examined this association by stratified age groups. Not surprisingly, the incidence rate of muscle loss was higher in older participants. In addition, the risk for muscle loss were notably higher in participants aged ≥60 years, particularly when they had both DM and CKD. A total of 210 (3.4%) cachexia events were noted during the follow-up. The study found th2at subjects with DM alone were associated with a 1.55-fold higher risk of cachexia compared to those without DM and CKD, and the risk of cachexia was markedly higher in subjects with the two conditions. No significant association between CKD and the risk of cachexia was observed. Also, the risk of all-cause mortality was significantly higher in subjects with DM alone than in those without DM and CKD.
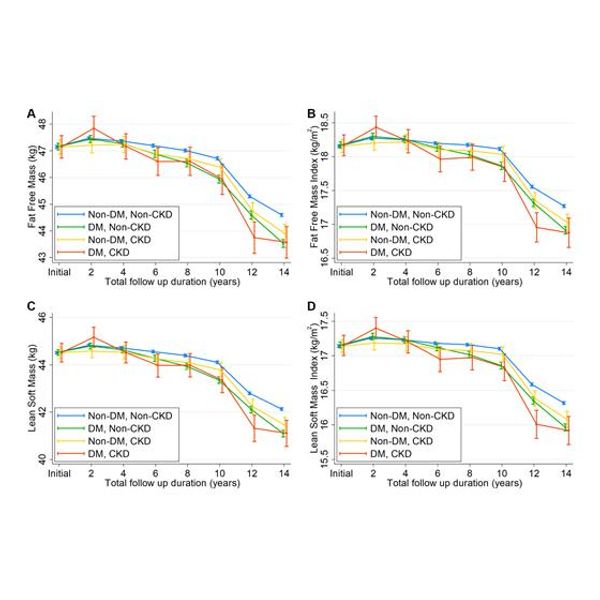
Figure 1: Changes in (A) fat-free mass, (B) fat-free mass index, (C) lean soft mass, and (D) lean soft mass index over follow-up time. Figure adapted from Lee C et al. Aging 2021, vol 13, doi: 10.18632/aging.203539
Total 460 (7.4%) subjects had muscle depletion. The decline in fat-free mass, FFMI, lean soft mass, and lean soft mass index was greater in subjects with DM alone than in those without DM and CKD. Similar findings were observed in subjects with CKD alone, although the magnitude of the decline difference was less than that in subjects with DM alone. It was observed that muscle depletion was associated with a 6.42-fold higher risk of death and the association was greater in individuals with cachexia. Moreover, it was observed that glycemic control did not contribute to the higher muscle depletion risk in individuals with DM and CKD.
As an alternative to blood glucose testing, recent studies shows that a short 30 days monitoring of glycated albumin should be examined. Albumin is the largest circulating protein in the blood. Glycated albumin refers to albumin attached to glucose and offers an advantage of monitoring average blood glucose over a short-term period of one month (as albumin replaces itself every 30-days). A rapid test for GA could be a significant benefit for patients to control diabetes and other related complications on a monthly basis. Epinex has patented a rapid test for Glycated Albumin (G1A) and is developing this test for clinical trials. G1A tests measures total albumin and glycated albumin exclusively, in a handheld device as a POCT (Point of Care Test) for doctors’ offices and clinics, and as an OTC (Over the Counter) test for general public use.
Reference: Lee C, Kim HJ, Chang TI, Kang EW, Joo YS, Kim HW, Park JT, Yoo TH, Kang SW, Han SH. Synergic association of diabetes mellitus and chronic kidney disease with muscle loss and cachexia: results of a 16-year longitudinal follow-up of a community-based prospective cohort study. Aging (Albany NY). 2021 Sep 16;13(undefined). doi: 10.18632/aging.203539.