

- Home
- Companies
- Navigate Surgical Technologies Inc.
- Articles
- Dynamic Surgical Guidance to Facilitate ...
Dynamic Surgical Guidance to Facilitate Dental Implant Placement
The long-term success of dental implant surgery is dependent, in part, on accurate planning and placement of the implant.1 Currently, there are many digital planning systems available to aid the clinician in pre-operative treatment planning, although the main challenge with these planning systems is to accurately transfer the digital plan to the clinical situation. Most systems involve taking a cone beam computed tomography (CBCT) or other three-dimensional scan of the patient, and then digitally placing implants using a software program.
Traditionally, static surgical guides are used to relate the digital planned position of the implants to the clinical situation. However, there are several drawbacks to static surgical guides. Specically, the surgical guide cannot be modied intraoperatively to adapt to chairside decisions that result in changes to the clinical plan. Furthermore, static guides are typically designed over the surgical site, and so there is some impediment to the visualization of the surgical field. Finally, the static guides have small but signicant distortions associated with them, resulting in an accuracy of implant placement that varies widely. Studies have reported wide ranges of deviations in implant placement relative to the planned position in both apico-coronal and angular dimensions for most commercially available systems.2-6 Inaccurate implant placement can result in short-term complications, such as damage to adjacent vital structures, as well as a long-term increase in implant failure.7-9.
A new technology to address these drawbacks is dynamic surgical guidance.10-12 Dynamic surgical guidance technology involves a computerized navigational system intended to provide assistance in both the planning (pre-operative) and the surgical (intra-operative) phases of dental implantation surgery. Dynamic surgical guidance provides two main modes of operation: preoperative case planning and intraoperative surgical treatment. In the preoperative phase, the system is first used to plan the dental procedure including the planned implant location within the CBCT image. During the planning phase, the clinician can select the implant system for each surgical site. Case planning can be done prior to the day of surgery, in which case the treatment plan can be saved into the case management database or, alternatively, the case can be planned immediately prior to surgery.
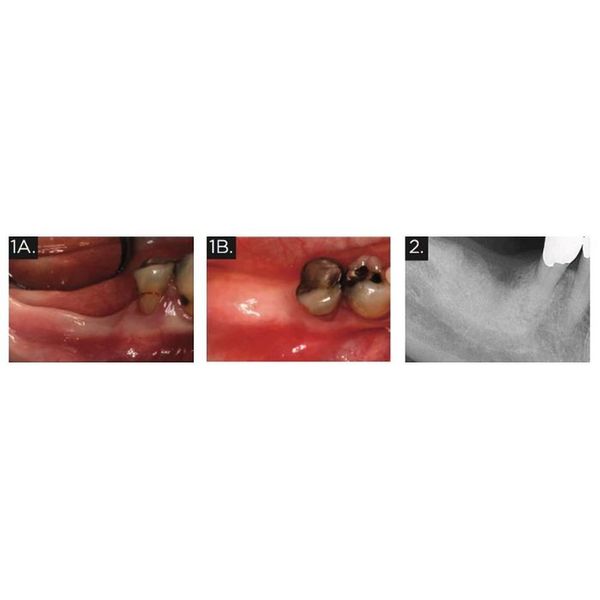
A 72-year-old Caucasian female presented to Cityview Periodontal Center with a missing #46. The patient’s chief complaint was the “desire to replace her missing tooth”. A comprehensive examination was conducted, including an intraoral examination, digital impressions, and radiographs (Figs. 1 & 2) . The radiographs identified that the inferior alveolar nerve was in close proximity to the planned location of the implant.
TREATMENT:
Multiple treatment options were presented to the patient, including placing two implants to replace #46 and #47. The patient chose to only replace #46 at this time. Due to the challenging nature of the case, it was decided to use dynamic surgical guidance for both the implant planning and surgical phases.
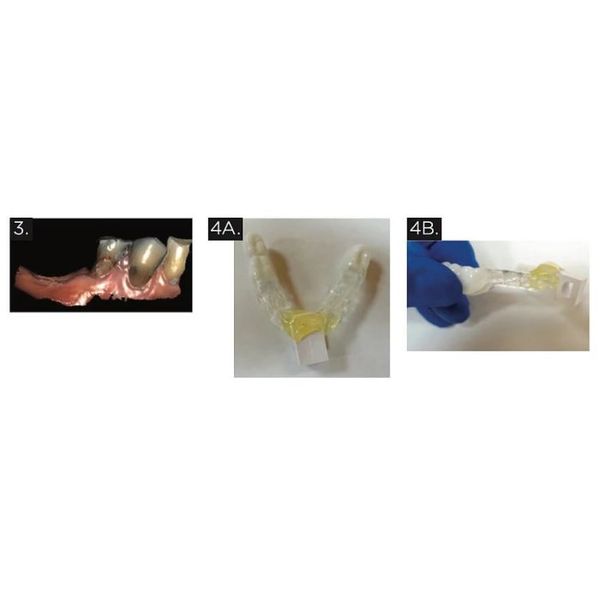
An imaging stent with radiopaque teeth was fabricated from the digital impression (Fig. 3) . In case the patient chose to replace #37 and #47 in the future, these teeth were also added to the stent. Then, a plastic marker that also serves to hold the patient tracker (called a fiducial) was added to the imaging stent, and a cone beam computed tomography (CBCT) scan taken with the imaging stent/fiducial in place (Fig. 4) .
IMPLANT PLANNING PHASE
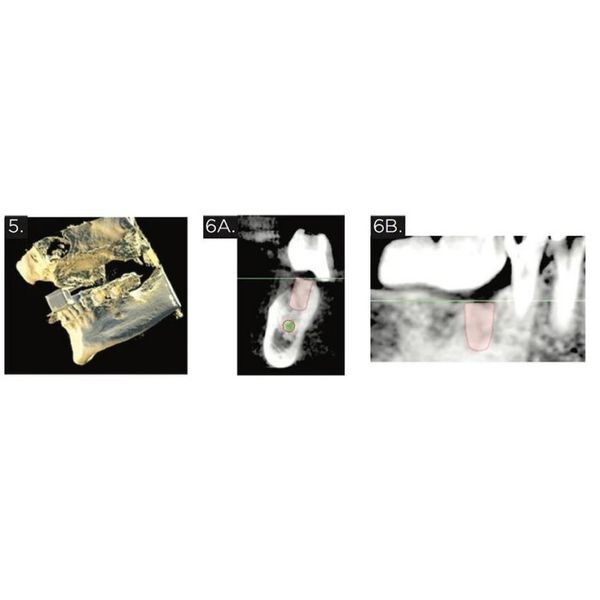
The CBCT images, with the radiopaque prosthetic plan visible in the scan, were uploaded into an implant planning software program associated with the dynamic surgical guidance system. Then, the ideal implant size and position was planned using the software, respecting the anatomical limitations of the area (Fig. 5-6) . The digital plan for the final implant position was confirmed and the patient was prepared for surgery.
PRE-SURGICAL SETUP PHASE
Immediately prior to surgery, the patient took 300mg clindamycin orally, and rinsed with 0.12% chlorhexidine rinse for one minute. The imaging stent was modied to eliminate the portion of the stent in the surgical area, and the tracking arm was attached (Fig. 7). Both the tracking arm and the handpiece (Fig. 8) contain black marking dots that can be identied optically by tracking cameras that attach to the overhead light (Fig. 9) . This setup constitutes the basis for the dynamic surgical guidance system, which is able to identify the drill position relative to the patient position intraoperatively.

SURGICAL PHASE
A full thickness flap was raised to the mucogingival junction. Then, the stent with the tracking arm was secured onto the patient’s anterior and left posterior teeth, and stability of the stent was veried. An osteotomy was prepared in #46 position using the recommended drills and sequence. The dynamic surgical guidance system was used throughout the surgical phase to identify the position of the drills within the patient’s anatomy using the CBCT scan images, and viewed on a screen behind the patient (Figs. 10 & 11). A Strauman SLActive 4.8 mm WN x 8 mm implant was placed successfully according to the dynamic surgical guidance plan, with adequate distance (>2 mm) from the apex of the implant to the inferior alveolar nerve canal. A 3mm healing abutment was placed and the ap sutured using 4-0 vicryl sutures. Final clinical photographs and a periapical radiograph were taken (Figs. 12 & 13) .

RESTORATIVE PHASE
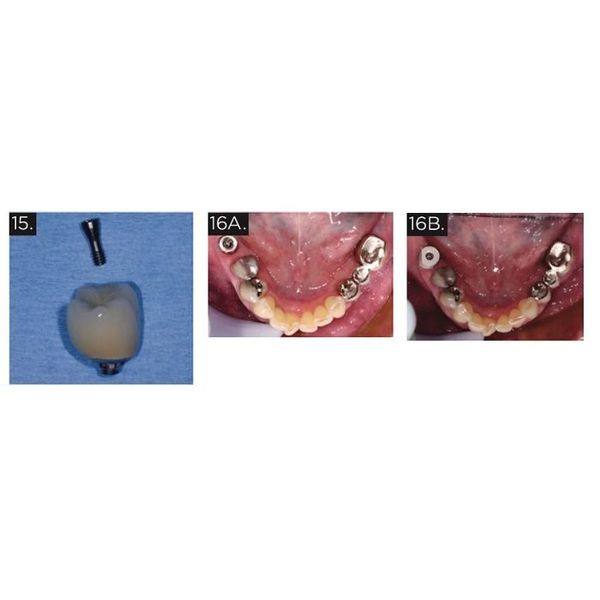
After approximately three months healing, the stability of the implant was tested using a reverse torque test. A peri-apical radiograph veried that the bone levels around the implant remained acceptable and that the implant was ready to restore (Fig. 14) . Digital impressions were taken using a Straumann Monobody scan body and the iTero digital scanner. A direct screw-retained #46 implant crown was made (Fig. 15) . The abutment screw was torqued to 35 N-cm (Fig. 16) . The occlusal access hole was filled with a Teflon tape spacer and an occlusal composite restoration (Fig. 17) .
CONCLUSION
Dynamic surgical guidance is a tool available to implant surgeons that has the potential to increase predictability of implant placement. The ability to visualize the dental implant drills within a three-dimensional view of the patient’s anatomy provides a major advantage in dental implant surgical technology. In this case report, dynamic surgical guidance was used to ensure safe, accurate, and efficient planning and placement of a dental implant in the posterior mandible in a challenging anatomic situation.