

- Home
- Companies
- LimFlow, Inc.
- Articles
- LimFlow Percutaneous Deep Venous ...
LimFlow Percutaneous Deep Venous Arterialization
What interested you in LimFlow, and how did you get involved in the PROMISE I trial?
Dr. Clair: Practicing vascular surgery, where a number of patients are evaluated for chronic limb-threatening ischemia (CLTI), you are guaranteed to have patients who are not candidates for percutaneous or surgical revascularization. These patients often have arterial systems open or identifiable to the ankle, with little to no flow in the foot, or what has been termed “desert foot,” progressive tissue loss, and prior unsuccessful attempts at stopping this progression. Previous surgeons have looked at arterialization of venous flow, but there had never truly been adequate proof of benefit. I was interested in finding out if there was any way to deliver oxygenated blood to the tissues of the feet in these patients, and venous arterialization offered an opportunity to do this. I had heard of percutaneous procedures for doing this and contacted the company early on as I had an interest and believed the concept had value for these patients.
Dr. Shishehbor: I became interested in LimFlow because I’m always looking for options to save my patient’s limbs, and I know the impact that amputation has on patients in terms of mortality and psychosocial elements, as well as the costs that it has to the health care system. I felt that this was cutting edge, something unique. I was able to engage in PROMISE I, and we have had some very good experiences. As a matter of fact, the first patient we treated with LimFlow was a woman with a prior amputation on the left leg. She was set to undergo an amputation on the right leg, but we were able to save it, and she is still walking today because of the LimFlow procedure.
How would you describe the learning curve?
Dr. Shishehbor: Early in my experience with the technology, I found it technically challenging, but like anything else, it becomes easier with practice. We’re also working globally with our friends in Italy, Singapore, and in United States to try to improve our techniques. The procedure used to take me 4.5 hours, and now a straightforward case can be done in 90 minutes. Again, it gets easier with experience, but some aspects of the procedure require a little bit more energy and commitment.
Dr. Clair: The learning curve is variable because of the variability of the venous anatomy, but gaining experience with LimFlow has also allowed me to train people better than I was initially. For example, we were initially gaining access in the lower leg, but it has become clear that if access can initially be gained in the plantar surface of the foot, the procedure can be much easier to complete. Additionally, we have learned that the delivery of oxygen to the tissues is not something that happens immediately upon creation of the arteriovenous communication; rather, it takes several weeks for the arterialized venous flow to deliver oxygenated blood to the tissue. An understanding of the venous anatomy of the foot, including the named venous branches and the locations of the valves, has proven valuable in standardizing the procedure and decreasing the time for completion of the procedure. There is still much to be learned, but there is no question that those learning this technique today are better at it than I was with the first of these procedures I performed.
Longer-term success for no-option patients can be defined by limb salvage, which cannot be reliably achieved without wound healing. In the PROMISE I and II trials, the primary endpoint is amputation-free survival, and this is our measure of long-term success. It is critical to understand that these patients require more attention than those undergoing standard arterial revascularization. Patients in whom the arterial system can be reconstructed have oxygen delivery corrected immediately; for these patients, it may take 4 to 6 weeks to achieve adequate delivery of oxygenated blood from the deep vein arterialization, and the physician caring for these patients needs to be meticulous in the follow-up of the new circulation and in the care of the wound.
How would you describe the patient population included in the PROMISE I trial?
Dr. Clair: The patient population in the PROMISE I trial might be the most thoroughly evaluated group of patients with nonreconstructible CLTI. They were vetted by an independent panel of vascular specialists to confirm that they had no revascularization option other than the LimFlow procedure. No other trial looking at treating patients with no alternatives to standard revascularization techniques has had an independent panel confirming this status. In addition, I would call this group of patients perhaps the most severe form of CLTI. I don’t think this population is comparable to any other group that has been studied before and I believe they are likely older, sicker, and with more severe peripheral vascular disease than any other group that has been studied before.
Dr. Shishehbor: These patients are also very passionate people. For many, it is more than just a risk because they are already scheduled to lose their leg, and they’ve been told there are no other options. They may have a lot of comorbidities—such as diabetes, chronic kidney disease, end-stage renal disease—and they’re complex cases. My experience with these patients has been challenging, rewarding, engaging, and emotional.
What are the key highlights from the latest 12-month data from PROMISE I?
Dr. Shishehbor: What we have seen from PROMISE I—amputation-free survival of 70%, freedom from amputation of 77%, and survival of 91% at 12 months—and our own center’s experience, has been incredible. This is a control group in which 100% of the patients were going to have an amputation or a palliative care situation, so any success is tremendous. Any time you can save a leg in a functional patient, in a patient that can otherwise walk, that is an impressive impact.
Dr. Clair: The PROMISE I trial provides evidence that deep vein arterialization with the LimFlow procedure is an option for limb salvage in this challenging group of patients. Deep vein arterialization offers an opportunity to prevent the progression to amputation we frequently see in this population, which appears to make up about 20% of patients with CLTI. As these patients are very fragile, the ability to perform this procedure as a percutaneous option is incredibly valuable in reducing the impact on these patients and offers the potential to limit their time in the hospital, and for many, it offers the only chance for them to keep their limbs and maintain their ambulatory status.
Beyond that, what is impressive and interesting about the PROMISE I 12-month data is the sustainability of the success. For those patients in whom we are able to get beyond the 3-month point, limb salvage is sustained out to 12 months. In addition, these patients seem to have what initially appears to be good survival as well. We are not seeing limb loss of any significance beyond the initial 2 to 3 months.
And finally, how is PROMISE II progressing?
Dr. Clair: PROMISE II has been enrolling despite the difficulties and challenges COVID-19 has imposed on the investigators, the facilities performing these procedures, and LimFlow’s ability to support the trial. We are now more than halfway through enrollment, and due to the adaptive statistical design the trial plans to enroll 60 to 120 “no option” patients.
Dr. Shishehbor: I’m honored to be a national Principal Investigator for PROMISE II along with my partner, Dr. Clair. We have an incredible team of investigators extremely committed to saving limbs, and I’ve learned so much from them. I’ve been very happy with the progress, and I look forward to the data coming out in the future.
PATIENT BENEFITS
Deep venous arterialization (DVA) has emerged as an alternative therapy for patients with no available revascularization option. Open and percutaneous techniques have previously been described to perform DVA with varying results.1,2 The percutaneous LimFlow System was developed to optimize the DVA procedure with purpose-built components that offer more consistent results. A high percentage of patients in my practice with chronic limb-threatening ischemia (CLTI) are diabetic, and they commonly do not have an open or endovascular target in their foot. I was unaware of DVA for many years and sadly many patients lost their limbs and suffered corresponding losses in quality of life. Having access to the LimFlow System has given me a new option to offer my no-option patients.
TECHNICAL EXPERTISE
Performing DVA with the LimFlow System utilizes standard endovascular techniques and is an accessible option for interventionalists already skilled in treating atherosclerosis causing CLTI. The LimFlow procedure can be summarized into the following steps: arterial access in the common femoral artery, venous access in the lateral plantar vein, artery-to-vein crossing, valvulotomy, extension stent graft deployment, and crossing stent graft deployment. As part of the PROMISE II trial, LimFlow introduced new devices to make artery-to-vein crossing and stent deployment much easier, and I was fortunate to be the first globally to use these new components.
AV Crossing: Arterial Catheter and Venous Catheter
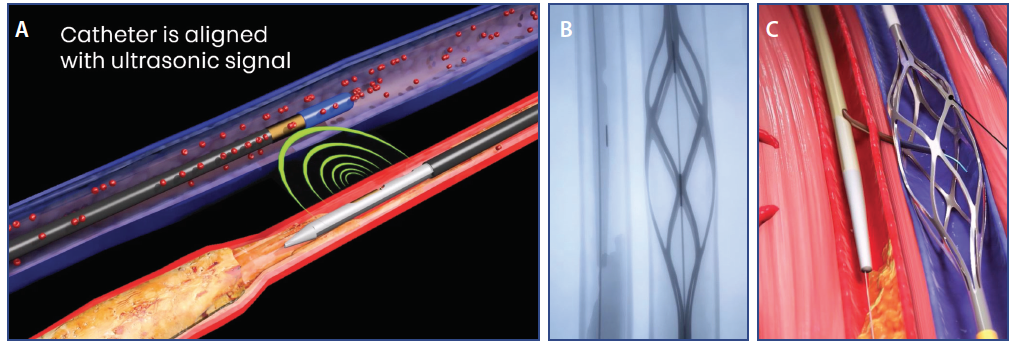
The previous LimFlow system used ultrasound-guided arterial and venous catheters to obtain optimal alignment during arteriovenous (AV) crossing. Ultrasound-guided crossing took more time for device alignment and crossing, and these additional steps had a longer learning curve to become proficient (Figure 1A). In the latest generation of the LimFlow System, the ultrasound components were replaced with new arterial and venous catheters that use standard fluoroscopic imaging to obtain optimal alignment, crossing, and wire retrieval (Figure 1B and 1C). The new venous catheter utilizes a radiopaque cylindrical mesh that is designed to hold the vein open and act as a target during AV crossing. The new arterial catheter is designed to be more ergonomic, flexible, and lower profile. These improvements are designed to make AV crossing easier because these new components operate in a familiar way to endovascular specialists. The first time I used the new venous catheter, crossing was completed on my first attempt as I visualized the needle enter the mesh of the venous catheter. The ergonomics and lower crossing profile (7-F to 6-F) of the new arterial catheter are designed to make it easier to track it to the arterial crossing point, and the greater crossing needle stability may allow for more predictable AV crossing. The new AV crossing devices and the use of direct fluoroscopic visualization instead of ultrasound are designed to avoid contrast injection and unnecessary manipulation in the tibial veins.
{kind=link}
Stent Graft Deployment
The initial LimFlow System used a pin/pull stent graft delivery system for stent graft deployment. Although a pin/pull system is easy to use, it has disadvantages. There is energy transfer through the catheter that makes deployment less precise, and higher forces are required to deliver longer stents. I was fortunate to be the first to use the new delivery system with the dial mechanism that deploys the stent graft in an easier and more precise way. The catheter tracks very well and goes into small, calcified arteries with ease. The new stent graft delivery system has also made it easier to deploy longer 150- and 200-mm stent graft lengths. For a self-expanding stent graft, it has very good radial force that helps maintain patency. In addition, the tapered LimFlow crossing stent is designed for optimal sizing for artery and vein.
Retrograde Valvulotomy Catheter
After completing AV crossing, the LimFlow Push Valvulotome is used to lyse the valves in the veins below the crossing point and into the foot. It is critical to completely lyse valves prior to stent deployment and to reach as distally as possible in the foot. The Valvulotome is opened by retracting its integrated sheath and only cuts in when pushed in a forward direction. There is a tactile and visual response when the Valvulotome is engaging valves. Complete treatment of valves below the crossing point allows for more complete stent graft deployment and uninhibited flow distally to the foot. Being over the wire and retrograde seems unnatural for vascular surgeons because we are used to passing the catheter retrograde and then pulling to perform valve lysis, making this a novelty and a great option.
CONCLUSION
The product and procedural improvements in the latest updates to the LimFlow System have made AV crossing easier and more reproducible, and stent graft deployment is more accurate and with long length implants. These improvements will make the therapy and the LimFlow System more easily adoptable by a greater number of physicians and will offer new options to no-option patients across a broad spectrum of specialties.
A percutaneous deep vein arterialization (pDVA) circuit typically matures in 4 to 6 weeks, at which point an acceleration in wound healing commonly occurs. During this initial period of maturation surveillance is mandatory to detect any changes in flow that may threaten the patency of the reconstruction and therefore wound healing. There are two main goals during follow-up, which differ from a regular arterial reconstruction. The first is to maintain patency, which is analyzed by duplex ultrasound (DUS) measurements and include peak systolic velocity (PSV), as recommended for regular infrainguinal bypasses, and volume flow (VF) measurements as recommended for arteriovenous (AV) fistulas.1,2 The second is to establish forward pressure for wound healing; this is evaluated with transcutaneous oximetry measurements of the foot in combination with DUS analysis of side branches that can potentially steal flow.
WHY USE VF MEASUREMENTS IN THE SURVEILLANCE OF pDVA CASES?
VF measurements are used in AV fistulas and can predict failure of the reconstruction when there is a sudden drop in flow or a certain threshold is passed. In a recent study we published, we analyzed the postoperative measurements in pDVA patients.3 The analysis showed us that the VF was a reliable predictor for flow when measured at the right place. A test-retest analysis showed that the diagnostic accuracy and reliability was high for measurements performed midstent and this is probably due to the laminar flow in the stent at this point and the standard diameter of the stent used in the measurement.
HOW TO BEST PERFORM THE DUS AND CALCULATE VF
In our study, to obtain the VF, the diameter of the vessel was measured with the calipers at right angles to the sample volume. Three pulse cycles on the spectral trace were selected, and the system automatically estimated the time-averaged mean and calculated the VF in mL/minute.
WHERE TO MEASURE THE VF
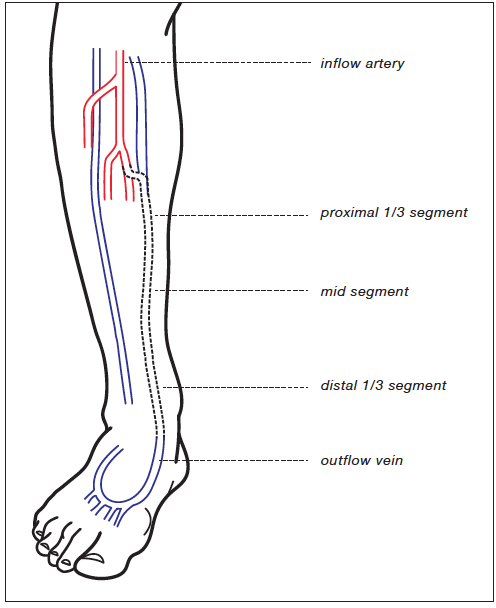
We recommend measuring the PSV and volume flow at five locations (Figure 1); the inflow—the popliteal artery (P3); the proximal one-third segment of the covered stents, the middle segment, and distal one-third segment of the stented vein; and at the distal outflow vein, > 3 cm distal to the lowest point of the covered stent. Besides this, we search for significant stenosis and for side branches in the outflow vein which potentially can steal flow. The VF found at the middle segment of the stent is interpreted as most reliable.
{kind=link}
CLINICAL INTERPRETATION OF THE MEASUREMENTS
An analysis showed that a VF value of < 195 mL/minute and a PSV value, < 55 cm/second was predictive for failure. A VF value of > 364 mL/minute and a PSV of > 99 cm/second was defined as predictive of patency.3 However, it should be noted that very high VF may indicate excessive shunting of flow and should also be monitored closely. There is a large difference between the values due to the small cohort, but when a sudden drop in value or a low flow exists, it is an indication for close follow-up or reintervention. The most reliable value is at the middle segment of the stented vein but care should be taken when interpreting these values.
CONCLUSION
After a pDVA, it is important to frequently evaluate the reconstruction because it needs 4 to 6 weeks for the arterialization to mature. The VF plays an important role in this evaluation, but a final judgment about the perfusion of the foot and an indication for reintervention should be based on a combination of the clinical evaluation, the DUS findings, and transcutaneous oxygen measurements.
Endovascular arterialization implies the placement of long, polytetrafluoroethylene (PTFE) covered stents. These stents secure the flow of oxygen rich blood from the arterial supplier to the venous donor vessel. Multiple past studies have shown that dual antiplatelet therapy (DAPT) is mandated when deploying extensive metallic scaffolds in lower extremity vascular beds.1 Although there are no randomized controlled studies specifically on this topic, we recommend this practice as baseline therapy.
Our own experience has led us to develop a protocol that entails the combination of ASA and clopidogrel (DAPT) as the initial combination therapy. Additionally, and once on formal DAPT, we order an adenosine diphosphate inhibition test aimed at measuring the clinical effect of such therapy. In the event that there is insufficient platelet inhibition (inhibition > 20%), clopidogrel is substituted with ticagrelor. Finally, if despite the previous regimens and with proven platelet inhibition, the patient has an unexpected, unexplained early stent thrombosis, once it is resolved (via thrombectomy and/or lysis) the patient will be optimized with an oral anticoagulant on top of the antiplatelet of choice.
FOOT SURGERY
The two main drivers for early foot surgery are infection and severe ischemic pain. Data from the ALPS study led us to believe that arterialization tends to improve tissue oxygenation after 4 to 6 weeks after surgery, so if we can stall, we will always err on the side of observational patience.2 Temporizing surgery driven by the above stated findings is to be as minimalistic as possible, but as effective as possible. Moreover, maximal tissue preservation is always intended, as some degree of tissue die back is expected in the first 2 to 3 weeks postarterialization.
The care after the hyperacute phase for the arterialized patient includes what we like to call “Toe and Flow Surveillance.” Due to the aforementioned extended time from arterialization to formalization of the foot procedures (an average of 4-6 weeks after deep vein arterialization) it is important for the patient to be seen by both specialties (vascular intervention [flow] and podiatric surgery [toe]) for close follow-up via weekly monitoring. This would include routine ultrasound surveillance of the arterialization performed by the “flow” team followed by monitoring of the wound site by the “toe” team to ensure no major changes in the wound status. Events that should raise suspicion with the clinician would include any significant changes in the noninvasive studies (including advancement of disease of the inflow vessels or significant drop in the arterialization flow volumes and peak acceleration times values), as well as any status change of the overall clinical condition. This may include but not be limited to changes in pain level, changes in the wound condition, edema, erythema, increased drainage or odor, and/or decreased ambulation. All of these can hint to a concern for underlying infection/ischemia and the need for early intervention or temporization.
Aggressive antibiotic management for any infection is a must, but understanding the changes (positive or negative) of existing wounds is crucial. The last concept is especially difficult for patients and family to understand, and they must be observant and vocal about any changes they witness. The primary goal is to preserve as much of the plantar surface as possible for shoe fitting and weight-bearing, with the overall goal of ambulation.
WOUND CLOSURE AND COVERAGE
In this particular patient population, it is very important to understand and be comfortable with avoiding primary wound closure or delayed primary closure. It should be avoided in all cases as the arterialized patient can experience prolonged lower extremity edema due to the robust increased blood flow to the extremity. This increased flow can place pressure at the closure site leading to wound dehiscence. It is best in this population to use scaffolds where needed in order to build up to a robust granular wound bed that can later be covered with a skin graft.
In terms of wound coverage, there are a few important factors to consider. First, what is the overall goal of the coverage and where on the foot is the wound located? Plantar wounds require more robust products for coverage than dorsal wounds. Are there anatomic structures needing coverage such as tendon, bone, or capsule? These would require the use of biologics indicated for exposed structures.
Second, it is important to ensure complete removal of the nonviable tissue and bone and that the wound is clear of infection. Immediate coverage postoperatively should be delayed for several days after any debridement to be able to not only have the ability to see the underlying tissue and how it responds to your debridement but also to ensure no lingering signs of infection remain. Obtain proper intraoperative cultures, and if you suspect bone involvement, always send a “clean” bone margin to ensure residual infection does not remain.
The split-thickness skin graft is a great means for final coverage of a large wound and should only be used once the wound presents with a healthy and robust granular wound bed.3 It may not be as durable on a weight-bearing surface of the foot given the mechanical forces applied. However, if the patient has proper accommodative shoes and or devices available, this will help to limit graft failure.
In our experience, the best postoperative management of the split-thickness skin graft is applying negative pressure wound therapy over the site to help bolster and assist with graft take. This is typically done up to postoperative day 5 followed by routine dressing changes with a dry sterile dressing every 2 to 3 days until healing has been achieved.
TOE, FLOW, AND GO
We have heard a lot about the “Toe and Flow” model,4 but the “Go” component may be just as important in the road toward limb preservation. What the “Go” component represents is true, functional limb salvage. This is achieved by having a clear surgical plan with the intention of tissue preservation as well as focusing on maintaining as much of the plantar surface of the foot as possible. Once healing has been achieved, the next step is to interface with an orthotist or prosthetists who can ensure transition to proper shoe gear to protect the foot and provide ambulatory assistance as needed.
Another important aspect of the “Go” concept is physical therapy and rehabilitation. It is our opinion that all patients are most successful after having had aggressive physical therapy and rehabilitation throughout the entire timeline of limb preservation. This best achieved by an initial inpatient acute rehabilitation stay followed by aggressive outpatient therapy once the patient has graduated from the inpatient rehab setting.
CONCLUSION
The combination of best practices after deep vein arterialization outlined above for “Toe, Flow, and Go” represent our latest developments in functional limb salvage and must be performed through close collaboration between multiple specialties.
Traditionally, chronic limb-threatening ischemia (CLTI) is considered the final clinical manifestation of peripheral artery disease (PAD), presenting with rest pain or tissue loss.1 PAD is described as a plaque-based, atherosclerotic big artery disease (BAD) starting with focal or multifocal lipid deposits inside the intima. However, especially in patients with diabetes mellitus (DM) or chronic kidney disease (CKD), we frequently observe the presence of small artery disease (SAD), spreading into the below-the-ankle arteries.2
CLTI patients can present BAD, SAD, or a combination of both entities. We can usually treat BAD with bypass or angioplasty, restoring a direct line of pulsatile blood flow to the foot distribution system. On the contrary, SAD is an untreatable disease, representing a barrier between the vascular system and tissues that can jeopardize the fate of the limb, in spite of any successful BAD treatment. For this reason, SAD is associated with poor clinical outcomes in terms of wound healing, time to healing, limb salvage, and survival.3
WHAT IS MAC?
Medial artery calcification (MAC) is independent from atherosclerosis and is correlated with aging, DM and CKD.4 MAC affects the arterial tree extensively, resembling “railroad tracks” along the silhouette of the arterial wall on plain radiography. In patients with DM and CKD, MAC is a powerful risk factor for cardiovascular events and death. Furthermore, MAC and an elevated ankle-brachial index, secondary to noncompressible ankle arteries as a result of MAC, are correlated with clinical symptoms of CLTI, such as foot ulcer, gangrene, and amputations.5
ARE SAD AND MAC TWO FACES OF THE SAME COIN?
Except for rare observations, SAD was never correlated with MAC.6 The pathophysiological mechanism by which MAC causes CLTI is unclear, essentially because MAC has been considered by most authors as a “nonobstructive” disease leading to arterial wall stiffening, loss of vasomotion, vascular aging, atherosclerosis, and plaque rupture.4,7 This literature suggests that MAC and CLTI could be correlated only through a robust enhancement of BAD development, fueled by MAC.
On the contrary, in our practice we frequently observe the coexistence of SAD and MAC in CLTI patients (Figure 1). For this reason we studied a cohort of these patients looking for the relationship between SAD and MAC and the clinical outcomes.8 The SAD score was obtained on the baseline angiographic study, whereas for MAC we proposed a new calcium score founded on plain foot radiograph (Figure 2).2,8
{kind=link}
{kind=link}
Figure 1. A 74-year-old woman with type 2 diabetes and first toe sufferance (F). On plain radiographs (A-C) the whole arterial tree is calcified with a typical railroad tracks pattern. Angiography shows occlusion of anterior tibial, peroneal, dorsalis pedis and medial plantar arteries. Posterior tibial and lateral plantar artery are diffusely diseased. The original metatarsal and digital arteries are severely diseased and substituted by new thin collateral vessels (D, E).
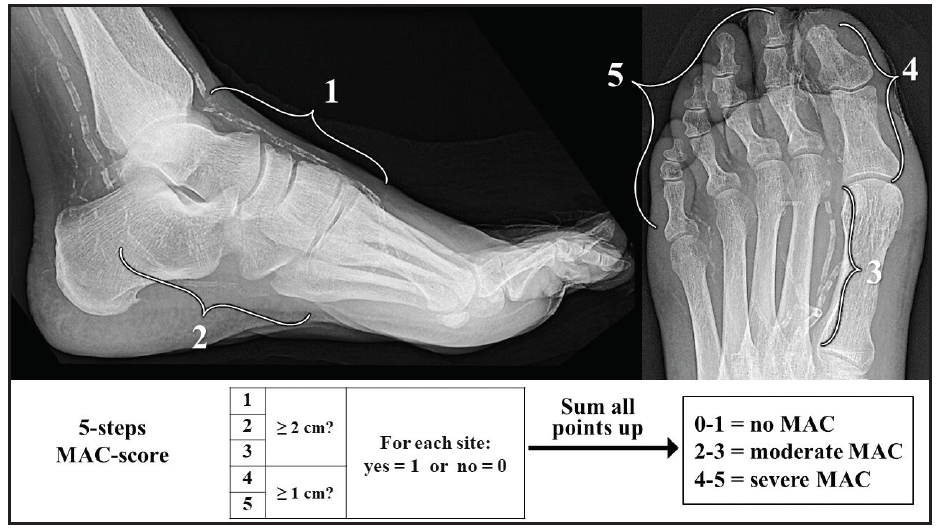
Figure 2. Upper part: Laterolateral and anteroposterior radiographic projections of the foot indicating the following five predefined vascular sites for assessment of MAC score: (1) dorsalis pedis artery, from the ankle joint to its disappearance inside the metatarsal bones; (2) lateral plantar artery, from the bifurcation of the posterior tibial artery to visible part of the distal plantar arch; (3) first metatarsal artery, from its proximal origin to the metatarsal-phalangeal joint line; (4) the first toe artery; (5) other significant vascular calcification in the other toe arteries, from the metatarsal-phalangeal joint line to the tiptoes. Lower part: Algorithm to obtain the final MAC score. Ferraresi R, Ucci A, Pizzuto A, et al. A novel scoring system for small artery disease and medial arterial calcification is strongly associated with major adverse limb events in patients with chronic limb-threatening ischemia. J Endovasc Ther. Published online October 15, 2020. doi: 10.1177/1526602820966309. Adapted by Permission of SAGE Publications, Inc.
MAC score was highly reproducible between different evaluators, with a high correlation coefficient (0.96). MAC and SAD score groups 0, 1, and 2 were defined as no/mild disease, moderate, and severe, respectively. The sensitivity and specificity of MAC score in predicting SAD was 100% and 98.1% respectively in SAD score group 0 and 2. For SAD score group 1, MAC score proved a sensibility and specificity of 99.1% and 92.7% respectively.
Patients with MAC and SAD scores 0 showed a more proximal localization of PAD obstructions, while patients with higher scores were more distal. These findings suggest the coexistence of the following two distinct obstructive diseases in CLTI patients: the well-known atherosclerotic BAD, causing a transmission failure of blood flow to the foot, and the SAD-MAC disease, leading to the below-the-ankle distribution failure. BTK arteries represent the overlapping field of these two different pathological entities.
According to clinical endpoints (complete healing, limb salvage, survival, foot surgical reintervention, redo-revascularization, and major adverse limb events), MAC and SAD scores demonstrated a highly significant difference when comparing group 0 with group 2. The comparison of group 0 and 1 and group 1 and 2 was significant in the majority of the clinical endpoints.
The multivariate analysis showed that MAC score was independently associated with redo surgical or endovascular procedures and major adverse limb events. Given the extensive experience of our interventional team with advanced endovascular and surgical revascularization techniques, we are convinced that severe SAD-MAC is the leading independent cause for patients not responding to traditional therapies. Repeated attempts for arterial reconstruction in these patients are doomed to fail and most likely major amputation will not be avoided.
LOOKING FOR NO-OPTION CLTI PATIENTS
In our study, nearly half of the patients presented a severe SAD-MAC score, and one third a moderate score, indicating SAD-MAC disease as a leading actor in contemporary CLTI. The widespread rising of age, DM and CKD in our societies drags behind an epidemic of predominantly SAD-MAC-CLTI patients for whom standard revascularization is not possible or ineffective, and the fate is poor. Patients with a severe SAD-MAC score are or will effectively become no-option patients for whom alternative treatments should be pursued as early as possible. Foot vein arterialization has shown to be the most promising limb salvage option for these patients.9-11