

- Home
- Companies
- KOPP Development Inc.
- Articles
- MRI Screening: What’s in Your Pocket?
MRI Screening: What’s in Your Pocket?
Magnetic resonance imaging (MRI) is a frequently used diagnostic imaging modality that may be an alternative to other types of radiologic imaging (e.g., computerized tomography, nuclear medicine imaging). It can detect soft tissue characteristics (e.g., inflammation), and because magnetic resonance (MR) uses a magnetic field and radio waves to produce images, it does not expose patients to ionizing radiation. Strict attention to MRI screening to prevent ferromagnetic objects and devices from reaching the MR scanner`s magnetic field is important for safe MRI. Significant injury can occur to individuals in the MR scanner suite if a ferromagnetic object or a device with ferromagnetic components is exposed to the magnetic field and radiofrequency energy of the MR scanner. To prevent injuries, MRI screening is done to identify ferromagnetic objects before patients, staff, or equipment enters the MR scanner room.
The Pennsylvania Patient Safety Authority was asked to review reports of MRI screening events submitted to the Authority. A query and analysis were completed of MRI screening events submitted from 2009 through 2017 through the Pennsylvania Patient Safety Reporting System (PA-PSRS), which identified 1,108 screening events. More than one-quarter of the events involved a device or object brought into the MR scanner room that was not considered safe for MRI. The most common objects or devices involved in MRI screening events were pacemakers (32.3%, n = 353 of 1,093 objects).
As medical technology advances, so do the risks for MRI screening events. It is essential to maintain high standards of MRI safety: research all medical devices for MR compatibility, educate patients and healthcare personnel regarding MR safety, and provide comprehensive MRI screening of all individuals entering the MRI suite.
A magnetic resonance imaging (MRI) scanner has strong forces that can move an internal ferromagnetic object (made of or having parts made of substances such as iron, nickel, and cobalt, which can be magnetized by exposure to a magnetic field). Further, the scanner can erase the memory or impair the function of a medical device and turn a ferromagnetic object into a projectile that can injure or kill. Because of this magnetic field and the associated radiofrequency energy, providing MRI screening for patients and staff is critical to their individual safety. Screening ensures that no ferromagnetic objects or objects (in or on anyone) that conduct electricity enter the magnetic resonance (MR) scanning area.
With the advancement of medical technology, the number of patients with external or internal medical devices is increasing and care within the MRI environment is changing. More complex procedures are being done with MRI guidance, often requiring more equipment to support the patient. These changes increase the potential risk for ferromagnetic devices entering the MRI suite and highlight the need for continued awareness and focus on MRI screening.
A request was made of the Pennsylvania Patient Safety Authority to provide an update to two previous articles (both from 2009) in the Pennsylvania Patient Safety Advisory1,2 with an analysis of recent data addressing MRI screening from the Pennsylvania Patient Safety Reporting System (PA-PSRS). This article addresses the identification and analysis of MRI screening events submitted from 2009 through 2017 and reviews strategies for keeping ferromagnetic objects and devices from reaching the MR scanner`s magnetic field.
Analysts queried PA-PSRS for MRI screening events submitted from January 1, 2009, through December 31, 2017. Criteria for identifying MRI events included the event type "error related to procedure/treatment/test," which includes event subtypes of radiology/imaging test problem or MRI safety violation, and event descriptions with terms like MRI and magnet. Analysis identified 1,448 events.
Analysts excluded 340 events involving adverse reactions to contrast, wrong-site (e.g., wrong side, wrong patient, wrong site, wrong procedure), scheduling issues, changes in patient`s clinical status (e.g., deterioration requiring intubation, vomiting, dizziness), other radiologic procedures (e.g., computerized tomography [CT], diagnostic x-ray), intravenous infiltrations and extravasations, incorrect results, patient injury caused by unintended physical contact with MRI equipment (e.g., bumps, bruises, skin tears), and inability to complete a study due to specific patient factors (e.g., claustrophobia, obesity).
The remaining 1,108 events were reviewed to determine the involved object or objects and/or device, whether the involved object or device was on or in the patient; the MRI zone where the event occurred or, in the case of a near miss, where the screening error was first identified; and level of harm designated by the facility as either an Incident (i.e., event resulting in no harm to the patient) or Serious Event (i.e., event resulting in harm).3
Classification of Objects and Medical Devices
MRI events were classified by whether the involved object or device would typically be used in the diagnosis, treatment, or prevention of disease (medical related) and its impact or potential risk to patients and staff when exposed to an MRI magnet, using the following categories:
- Ferromagnetic objects external to patient and staff that are brought within close proximity to the MRI magnet and have the potential to become projectiles when pulled towards the magnet.
- Ferromagnetic implants and/or foreign bodies within patients that are at risk of dislodgement because of magnetic translational and rotational forces.
- Medical devices that are at risk for malfunction or loss of data memory when exposed to the MR scanner.
- Objects that have thermal risk associated with exposure to the MR scanner`s radiofrequency field.
The following terms were used to categorize involved items (i.e., objects, devices):
- External—describes a nonmedical object or medical device that is outside of a person; may be attached to or on the skin
- Internal—describes a nonmedical object or medical device that is implanted (i.e., inserted or grafted into the body for prosthetic, therapeutic, diagnostic, or experimental purpose4) and/or within a person
- Medical device—machine, instrument, or implant intended for use in the diagnosis, treatment, or prevention of disease
- Active medical device—any medical device relying on a source of electrical energy to function (e.g., hearing aid, infusion pump, pacemaker)
- Passive medical device—a medical device that functions without electric power (e.g., cane, tissue expander, stent)
- Nonmedical object—any object that is unintended for use in the diagnosis, treatment, or prevention of disease
External medical devices and nonmedical objects were further grouped by commonality. External medical devices were categorized as disposable medical supplies, medical equipment, patient-specific medical devices, or medical instruments. External nonmedical objects included clothes, wearable items, and pocket items.
Classification of MRI Zones
MRI screening events were categorized by the regions, or zones, where the event was initially identified or occurred. Zones defined according to the American College of Radiology`s 2013 MRI guidance5 are summarized as follows:
- Zone I: all areas outside of the MRI suite accessible to the general public.
- Zone II: the interface between Zone I (uncontrolled) and Zones III and IV (strictly controlled).
- Usually where the patient is greeted, the patient history is obtained, and the MRI screening is completed.
- May include the reception area, changing rooms, and restrooms.
- Under the supervision of MR personnel.
- Zone III: free access by unscreened personnel or entry of ferromagnetic objects or equipment with ferromagnetic parts could lead to serious injury or death from interactions between the individuals or objects/equipment and the MR scanner environment (i.e., static magnetic field).
- Access is physically restricted for the general public and non-MR personnel, using a locking mechanism.
- Only MR-safety-trained MR personnel have free access. Level 1 MR personnel have had, at the minimum, MR training to ensure their own safety as they work in Zone III. Level 2 MR personnel have extensive training and education in MR safety issues.
- All access to Zone III is controlled and supervised by MR personnel who are charged with ensuring adherence to MR safe practices for the safety of the patient, personnel, and MRI equipment.
- Zone IV: Contains the MR scanner magnet and has the strongest magnetic field.
- Always located within Zone III because the magnetic field from the scanner`s magnet defines and creates the existence of the Zone III region.
- Clearly demarcated as a hazardous region due to the strong magnetic fields.
- Clearly identified with a red light and a red lighted sign with the words, "The Magnet Is On," which should be illuminated at all times.
- MR level 2 personnel should have direct visualization of access pathways into Zone IV.
Events that involved objects or devices brought into Zone IV were categorized as projectile (when the involved object or device was pulled towards the magnet) or nonprojectile.
Classification of Harm
Narratives were reviewed for accounts that described—
- Patient and/or staff injury; the event occurred in Zone IV
- Adequate screening of known devices deemed MR-safe (does not conduct electricity and is nonmagnetic6) or MR-conditional (tested under nonclinical conditions with specific conditions identified under which the device can be safely scanned6) but the patient experienced discomfort (e.g., burning, pain, sensation of object movement) when imaged; the event occurred in Zone IV
- Appropriate screening was done but an accurate patient history was unavailable, incomplete, or not provided; there was no known patient harm and the event could have been identified in any zone
- Patient had a known history of an internal or external device or object but appropriate prescreening did not occur; there was no known patient harm and the event could have been identified in any zone
- MRI screening form was not used or was incomplete but the patient was found to have no internal or external ferromagnetic objects or devices; there was no known harm and the event was identified in Zone I, Zone II, or Zone III
Of the identified 1,108 MRI screening events, the reports range from uncompleted MRI screening forms to ferromagnetic projectile events causing patient injury.
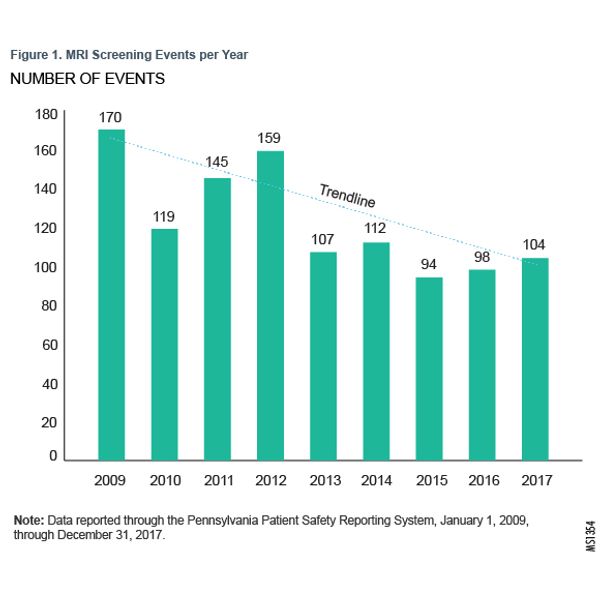
Analysis of MRI screening events over time determined that the number of reports has trended downward over the past 9 years. Figure 1 shows the number of screening events per year.
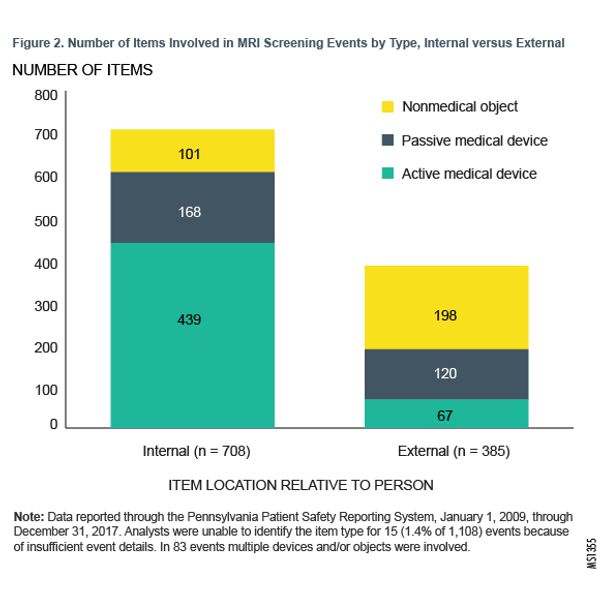
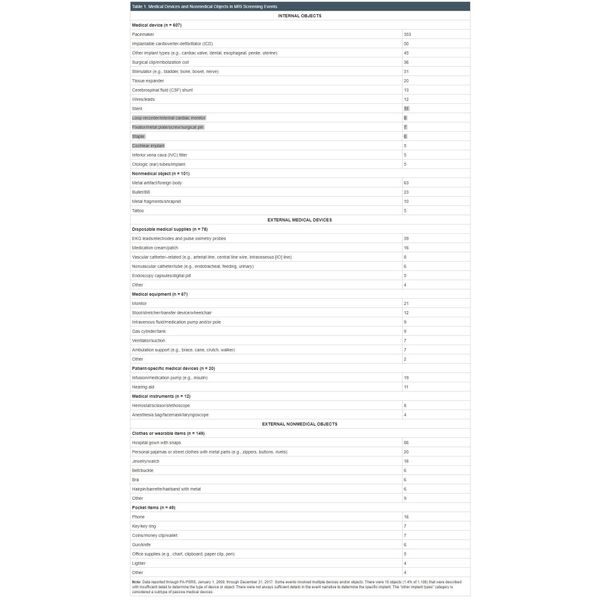
Of the 1,108 MRI screening events, 83 events involved two or more objects and/or devices. There were 15 events (1.4% of 1,108 events) that had insufficient event details to determine the type of device or object involved. Figure 2 shows the number of items based on the item type and location relative to the person. Of the MRI screening events with identifiable objects or devices, 64.8% (n = 708 of 1,093) involved internal medical devices and nonmedical objects; the most frequently involved items were pacemakers (32.3%, n = 353 of 1,093).
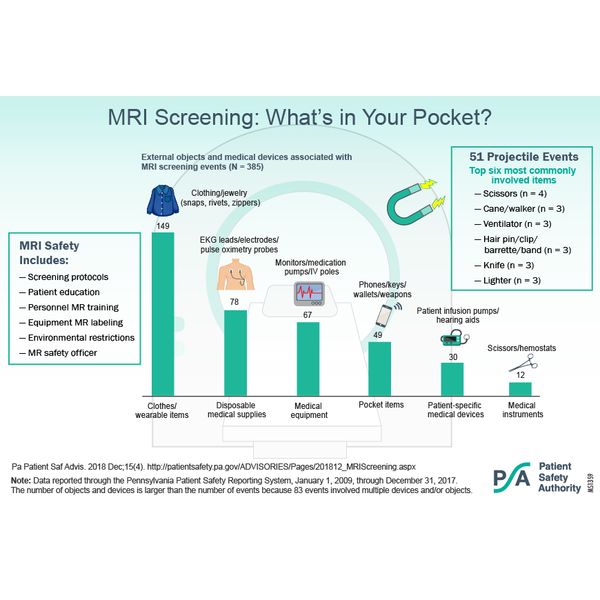
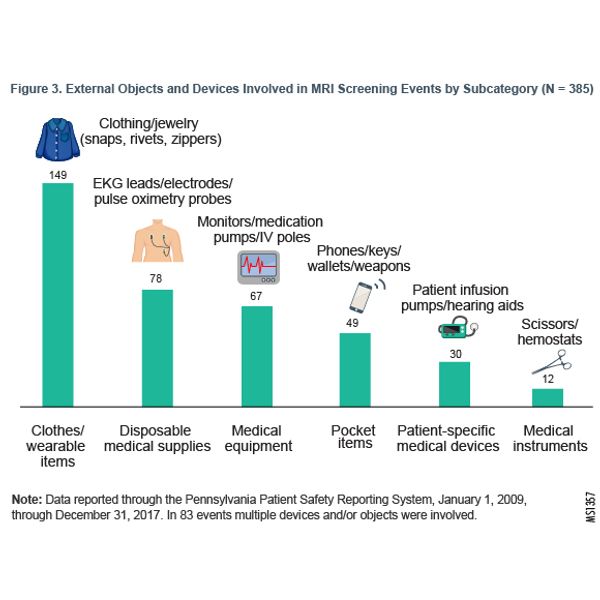
More than one-third (35.2%; n = 385 of 1,093) of events involved external objects, carried in by or attached to the patient or healthcare staff. Figure 3 shows the number of external objects based on commonality.
MRI screening events occurring in Zone I, Zone II, and Zone III were near misses (events that did not reach the patient and/or the involved ferromagnetic item was not exposed to the effects of the MR magnet) while events occurring in Zone IV may or may not have reached the patient.
Typical events by zone are described as follows:
Zone I
- The MRI prescreening form was not completed correctly or at all.
- Ordered MRI studies that were cancelled before the patient arrived in the radiology department. The event was generally noted when prescreening by review of the medical record and/or by patient interview identified that the patient had an implanted or external device that was not considered MR-compatible.
- The patient was known to have a possible ferromagnetic device or object but clearance criteria were unmet (e.g., metal fragments and orbital x-rays were not completed, patient had a pacemaker but there was no investigation completed regarding MR-compatibility).
Zone II
- The patient (typically an outpatient) arrived to the reception area or waiting room with a prescription for MRI imaging and review of an MRI screening form and/or patient/caregiver interview identified that the patient had an implanted or external device that was not considered or known to be MR-compatible.
Zone III
- The patient (typically an inpatient) was transported or brought into Zone III and review of an MRI screening form, the medical record, patient interview, and/or a physical finding (e.g., shape of a pacemaker on a patient chest was visible) identified that the patient had an implanted or external device that was not considered or known to be MR-compatible.
Zone IV
- Nonprojectile—
- An unknown (i.e., unknown to MR personnel) object or device was seen during the initial MRI imaging and the study was stopped.
- The patient had a known or unknown object or device thought to be MR-safe or MR-conditional and expressed that he or she had pain, burning, vibration, or a feeling of movement near the site of the object or device when imaged, so the study was discontinued.
- The patient had a known device that was thought to be MR-safe or MR-conditional and was found, either at the time of imaging or at a later date, to have malfunctioned or required interrogation.
- A ferromagnetic object was brought into the magnet room but was identified and removed from the room before it became a projectile.
- Projectile—
- A ferromagnetic object was brought into Zone IV and was pulled towards or into the magnet; the object might have come in contact with the patient or staff.
Figure 4 illustrates the number of events by zone.
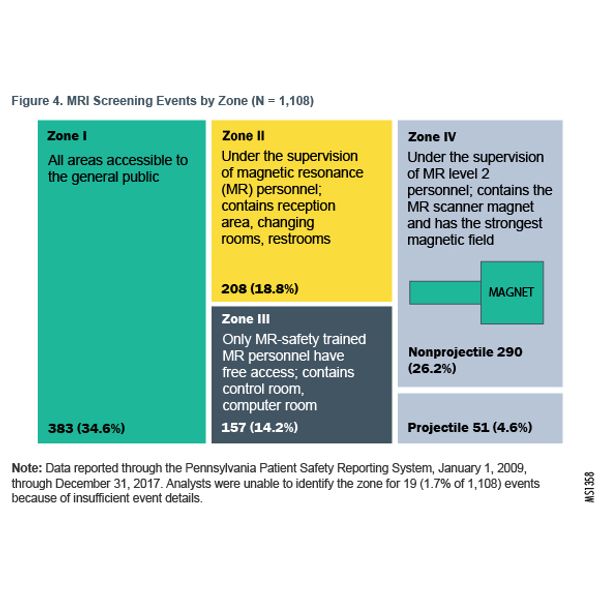
Of the events involving projectiles, 10 of the 51 projectiles (19.6%) struck either a patient or a healthcare provider. In three projectile events, the object did not strike a person but instead caused discomfort to the patient when either pulled from the grasp of the patient or when the patient was propelled towards the magnet with the object.
Events by Harm
Of the 1,108 events, 5 were designated as Serious Events and the remainder (99.5%, n = 1,103 of 1,108) as Incidents. The five Serious Events occurred as follows:
- One was related to a nonmedical object projectile
- One led to a thermal injury from an external medical device
- Three led to malfunction or displacement of an internal medical device
Events by Quality of Screening/Patient History
There were also 105 events reported based solely on the quality of the screening and/or clearance. Those events included narrative reports of screening forms that were either not used or not completed correctly and of clearance issues related to a patient history of a known internal medical device or nonmedical object, but preliminary screening images (e.g., x-rays, CT scan) were not ordered or an investigation of MRI compatibility information was not completed.
Examples of MRI Screening Events
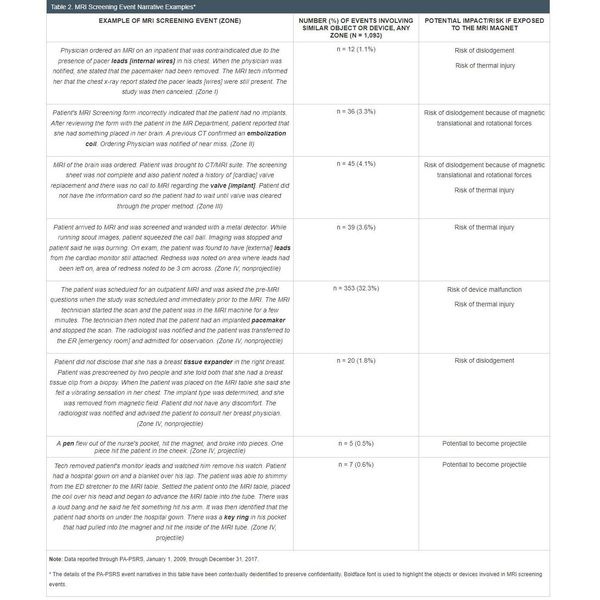
Examples of MRI screening events, the frequency of the objects involved, and the potential impact from exposure to the MR scanner can be found in Table 2.
Contributing Factors
Review of event details determined that multiple factors contributed to the MRI screening events:
- Screening forms were not completed or not fully completed either because of an oversight, staff unfamiliarity with the form, or a poorly designed form.
- Patients had known history of an internal medical device but there was either no investigation or not enough time to determine whether the medical device was MR-safe or MR-conditional—either because of an oversight, unfamiliarity with the process for investigating MR compatibility, or a delay in communication to the MR personnel by non-MR personnel (e.g., patient with a pacemaker with no documentation of MR compatibility).
- Patients had a known history of exposure to metal (e.g., metal worker, welder) but preliminary radiology screening was not ordered or completed because of an oversight or an unfamiliarity with the process for screening prior to MRI (e.g., patient who works with metal not receiving pre-MRI orbital x-ray imaging).
- Patients had internal or external medical devices but failed to disclose having a device during screening either due to poor recall or misunderstanding of the definition of terms such as "implant." A few event narrative details included examples of patients denying they had implants—because they misunderstood the term—but acknowledging, either during screening or after exposure to the MR magnet, that they had a battery in or on their bodies.
- Patients failed to disclose having exposure to metal due to poor recall or lack of knowledge regarding having internal metal artifacts and/or foreign bodies.
- External devices or objects reaching Zone III or Zone IV because the patient or non-MR personnel forgot they had ferromagnetic objects on them, were unaware of a device`s or object`s ferromagnetic properties or components, or did not understand the strength and potential impact of the magnet.
Limitations
This analysis has limits. The data reported through PA-PSRS are subject to the limitations of individual and facility reporting practices, including variations in quality and quantity of narrative details, frequency of reporting, and interpretation and designation of harm scores.
Analyst use of search terms specific to MRI screening may have limited identification of radiofrequency burns (i.e., search terms such as radiofrequency and burn were not included in the query).
Analysis was also limited by the need to interpret narrative details to categorize the zone of the event occurrence, because the specific zones were not always identified by the reporter.
The interpretation of whether an event "reached" the patient was limited to event details that described a patient with a ferromagnetic item on or in them being exposed to the magnetic field. Event descriptions did not always include enough details to determine outcomes for events "reaching" the patient, such as delays in diagnosis, further imaging, increased length of stay, or additional healthcare costs.
MRI is a diagnostic imaging modality that is used frequently and is safe when care is taken to prevent injuries from ferromagnetic objects.7 However, injuries related to the magnetic field of the MR scanner can occur when a ferromagnetic object or device is pulled towards the scanner`s magnet, causing the object to become a projectile with the potential to strike a patient, staff, and the MRI scanner. The magnetic field can also cause dislodgement of ferromagnetic internal implants (e.g., cochlear implants) or foreign bodies (e.g., shrapnel), and cause devices with ferromagnetic components (e.g., pacemakers) to lose stored data and/or malfunction. Thermal burn injuries from exposure of devices or objects to radiofrequency energy can also occur.
Other safety concerns specifically associated with projectiles are the potential for damage to the MR scanner and the need to turn off, or "quench," the magnet in response to the event. Quenching the magnetic involves releasing a cooled gas that can lead to displacement of oxygen in the room if not appropriately ventilated, which can cause loss of consciousness and death for anyone in the MR scanner room. Quenching the magnet also can cause significant damage to the scanner. Removing projectiles from the MR magnet, repairing the magnet, and restoring function of the MR scanner may take days or weeks after an event, leading to costly service calls and delays with patient imaging.
MRI screening to prevent ferromagnetic items reaching the magnetic field usually involves completion of an MRI screening form, including a medical history and follow-up verbal interview(s) by MR staff immediately before patients or staff access the MR scanner room. The interview is a safeguard to verify the accuracy of the information reported on the screening form and to confirm there are no ferromagnetic objects or devices, internal or external to individuals entering the MR scanner room.
Analysts found that fewer reports of MRI screening events have been submitted through PA-PSRS over the past five years, a possible reflection of focused attention and resources on MRI screening. However, it is important to recognize that there are more potential opportunities for MRI screening events because of the increasing number of patients with implanted electronic medical devices as well as increased use of medical equipment and supplies in the MRI environments (e.g., interventional procedures completed with MRI guidance, MRI procedures done under general anesthesia).8
Diligence to MRI screening remains critical to the safety of everyone—patients, accompanying family members, and healthcare staff—entering the MRI environment. Without close attention to MRI screening, patients and staff are put at risk of injury or death from projectiles, medical device malfunctions, and internal object displacement when ferromagnetic objects are exposed to electromagnetic forces.
Joint Commission has issued diagnostic imaging environment of care (EC) standards regarding MRI safety. The standards include the management of MR safety and security risks, including managing the risk for patients with medical implants, devices, or embedded metallic foreign objects and the risk associated with ferromagnetic objects entering the MR scanner room.9 Strategies for preventing ferromagnetic devices and objects from reaching Zone III and Zone IV are outlined below.
Strategies for Preventing Ferromagnetic Objects from Reaching Zone III and Zone IV
The following are strategies recommended by Joint Commission, the American College of Radiology, and other organizations supporting MRI safety for preventing ferromagnetic medical devices and nonmedical objects being brought into the magnetic field of the MR scanner.
MRI Personnel
- Designate an MR safety officer and/or medical director responsible for ensuring that MRI safety policies and procedures are in place and monitored for compliance5,10
- Have two levels of MR personnel who function under the direction of the MR medical director5
- Level 1: Personnel have passed minimal safety education training to ensure their own safety as they work within Zone III
- Level 2: Personnel have had extensive training and education in the broader aspects of MR safety issues
Non-MRI Personnel
- Provide MRI screening education for non-MR personnel who are ordering, scheduling, and/or sending patients for MRI procedures
- Provide MRI training for non-MR personal who are frequently in the MRI environment, such as surgical, transport, cardiac catheterization, anesthesia, environmental, maintenance, and emergency response staff8
Patient Education
- Provide information to patients and/or caregivers when scheduling an MRI such as the following:
- Risks and benefits of MRI
- Importance of completing MRI screening form
- Importance of providing a complete medical history, including any internal medical devices or nonmedical objects, exposure to metals, use of medication patches, and previous imaging11
- Clarification of medical terms such as "implant"
- Reminder to bring any medical device information and/or implant cards, if applicable11
- Expectations for the day of the MRI procedure such as the following:
- Need to change from street clothes (i.e., clothes with metal zippers, snaps, rivets) into a metal-free hospital gown, and removal of all objects with metal (e.g., jewelry, coins, cell phones) before entering the MR scanner room11
- Notification of MR personnel of any tattoos or nonremovable body-piercing jewelry8
- Potential of body scanning with a ferromagnetic detection system (FMDS) or strong magnet
- Availability of a patient call system in the MR scanner for use in the event of an emergency or patient discomfort11
MR Safety Culture
- Develop and implement policies to ensure that all MR safety events, including near-miss events, are reported in a timely manner to the medical director or MR safety officer and to other parties, such as the U.S. Food and Drug Administration (FDA), if applicable5,10
- Develop and implement policies that use MR safety events for quality improvement efforts5
Screening Process
- Create screening processes and forms for patients, non-MR personnel, and MR personnel that are essentially identical5
- Screen all patients and non-MR personnel for ferromagnetic or conductive medical devices and nonmedical objects internal or external to their bodies5,8,10
- Complete MRI screening for non-emergent patients onsite by two different individuals, one screen by level 2 MR personnel and one of the two screens done verbally5
- Develop processes for patients undergoing emergent scans and accompanied by non-MR personnel that allow for MRI screening to be completed once instead of twice, provided the screening is done by level 2 MR personnel5
- Interview patients and review their medical records, including previous radiologic or MR imaging, to determine the presence of any internal medical devices or nonmedical objects5,8,10
- Level 2 MR personnel physically examine patients for scars or deformities that may indicate internal medical devices or nonmedical objects or foreign bodies when a reliable patient history is unavailable and the MRI procedure cannot be reasonably delayed5
- Ensure removal of all metallic personal belongings and/or devices from every individual before they enter Zone IV, including cell phones, jewelry including body piercings (if removable), metallic medication-delivery patches, cosmetics containing metallic particles (e.g., eye makeup, nail polish), contraceptive diaphragms, hearing aids, clothing with metallic fasteners (e.g., underwire bras, clothes with zippers, rivets, snaps, or buttons) and hair barrettes/clips5,8
- Check all internal medical devices for MR compatibility8
- Develop a process for times when written documentation of MR safety status for an internal medical device by the manufacturer or by independent testing is unavailable. The process should include a discussion by the radiology and medical team about the risks and benefits for the MR imaging specific to the patient, with the final decision to proceed or not determined by the radiologist8
- Develop protocols and patient-specific plans for safely monitoring patients who are unable to communicate and/or sense pain or burning (e.g., patients who are anesthetized, sedated, very young, or have altered mental status)5
- Ensure the MR system is equipped with and patients are instructed on the use of an MR-safe device (e.g., call bell) in the scanner for alerting MR personnel of an emergency or discomfort
- Develop policies and training for scenarios, such as MR imaging of patients, prisoners, or parolees wearing ferromagnetic security devices; emergency service personnel (e.g., firefighters, police, security) responding to an emergent call requiring access to Zones III or IV; and non-MR healthcare providers responding to a cardiac or respiratory arrest in Zones III or IV5
- Designate an area outside of Zone IV where a patient can be rapidly moved for cardiopulmonary resuscitation (CPR)
Environment
- Provide gowns free of metal fasteners and private facilities for all patients to change out of personal/street clothes5,8,10
-
Restrict Zone III and Zone IV access for all persons not trained in MR safety or screened by MR trained personnel5,9
- Physically restrict Zone III and Zone IV access with a reliable, physically restricting method, such as a passkey locking system (use of a combination lock is discouraged)5
- Ensure restricted MRI areas (i.e., Zone II, Zone III, Zone IV) are controlled by and under the direct supervision of MR-safety-trained personnel5,9
- Ensure that all MRI areas are clearly identified as Zone III and Zone IV, demarcated, and clearly identified as being potentially hazardous5
- Ensure that Zone IV is clearly marked with a red light and lighted sign indicating that the magnet is always on5,9
- Provide level 2 personnel direct visualization of the access pathway to Zone IV either by line of site or by video monitors5
- Use FMDS devices only as an adjunct to thorough MRI screening (use of common metal detectors is not recommended)5
Equipment
- Do not allow equipment or medical devices containing ferromagnetic parts within the five-gauss (5 G) line (the line that delineates the boundary between areas where the MR system`s static magnetic field strength is greater than 5 G) unless tested by the manufacturer and labeled as MR-safe or MR-conditional for the facility`s specific MR environment5,8,10
- Provide clear documentation of MR-safe or MR-conditional devices (i.e., personnel should not assume that a device or equipment is MR safe or MR conditional)5
- Ensure that all equipment or medical devices used in the MRI environment are labeled with the appropriate MR safety label8,10
- Maintain an up-to-date list of all MR-safe and MR-conditional equipment8,10
- Use a strong magnet or hand held FMDS to test all unknown external devices or objects prior to entry into Zone III8
Analysis shows that the number of reported MRI screening events submitted from Pennsylvania healthcare facilities has decreased, possibly as a result of focused attention, education, and informational resources on MRI safety; but the increasing number and variety of internal medical devices, nonmedical objects, and medical equipment makes determination of MR compatibility an ongoing challenge.
Development and implementation of thoughtful policies are important to support continued enforcement of MRI safety protocols. Careful and conscientious attention to MRI screening can prevent injuries and save lives.