

- Home
- Companies
- LimFlow, Inc.
- Articles
- The Evolving Role of Percutaneous Deep ...
The Evolving Role of Percutaneous Deep Venous Arterialization
The increasing incidence of peripheral artery disease (PAD) is occurring globally as populations age and rates of diabetes, obesity, and renal disease increase.1-3 Although most of these patients have no symptoms, when the disease progresses to its most advanced form, chronic limb-threatening ischemia (CLTI), there is a significant risk for limb loss. Despite the fact that our revascularization options have improved over the last 20 years, a significant portion of patients with CLTI do not respond to available therapies, and a large group of patients with CLTI (15%–20%) are not candidates for standard revascularization therapies.4,5 Managing these no-option patients with conservative therapy and wound care has been disappointing, with wound healing in only 10% to 20% at 1 year.6 The unmet need for better outcomes in these patients has increased interest in the surgical technique of venous arterialization, which was first attempted more than 100 years ago with mixed results7,8 and has led to the development of the purpose-built LimFlow System for percutaneous deep vein arterialization (pDVA).
The LimFlow System includes devices specifically designed to easily achieve successful crossover from artery to vein, antegrade disruption of the valves, and delivery of a dedicated conduit to assure diversion of flow into the venous system and exclusion of more proximal branches to provide pressurized arterialized venous flow into the foot. Early experience with the LimFlow System has proven promising. The recently completed PROMISE I United States early feasibility study included 32 no-option CLTI patients who were indicated for major amputation. The study reported a high rate of major amputation-free survival (74%) and positive wound healing progression, with 67% of patients healed or healing at six months.9 These highly promising early results and the availability of a purpose-built system has allowed for more widespread adoption and the initiation of the ongoing PROMISE II United States pivotal study, which will evaluate the safety and effectiveness of the LimFlow System for pDVA in 60 to 120 no-option patients. As Co-Primary Investigator of the PROMISE II study, I am fortunate to have the LimFlow System as a potential option for my no-option patients and have seen firsthand its impressive effect on patients who were headed for amputation. Hopefully, by standardizing equipment, technique, and endpoints, LimFlow’s pDVA system will prove to be reproducible, safe, and successful in dealing with no-option CLTI patients.
A 4-STEP FLOWCHART FOR SELECTING NO-OPTION CLTI PATIENTS FOR pDVA
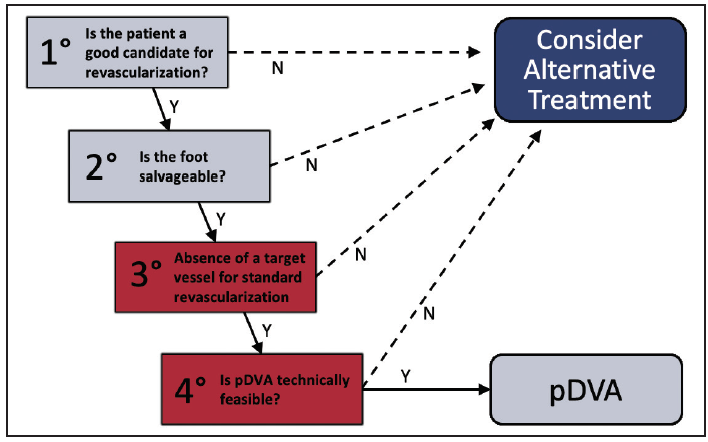
According to the Global Vascular Guidelines, all evidence-based revascularization in patients with CLTI must be managed considering patient risk, limb severity, and anatomic patterns of disease.1 pDVA is not an exception, and Figure 1 shows the 4-step flowchart for deciding whether a patient is or is not a candidate for this procedure. The first and second steps are similar to other standard revascularization procedures: a potential pDVA candidate must have an acceptable life expectancy and quality of life with the target of wound healing and maintaining the ability to walk. As a minimally invasive procedure, pDVA can be proposed to a patient who is unfit for open surgery but is a good candidate for endovascular revascularization. The third step is the key point in deciding between a traditional “arterial” approach or pDVA; if there isn’t a good target vessel with a reasonable chance of restoring perfusion to the foot and healing the wound, pDVA can be considered.
{kind=link}
Finally, the fourth step is to assess the technical feasibility for pDVA by confirming there is a suitable target artery to provide inflow to the pDVA circuit and suitable veins in the foot to arterialize and enable outflow.
WHO IS A NO-OPTION CLTI PATIENT?
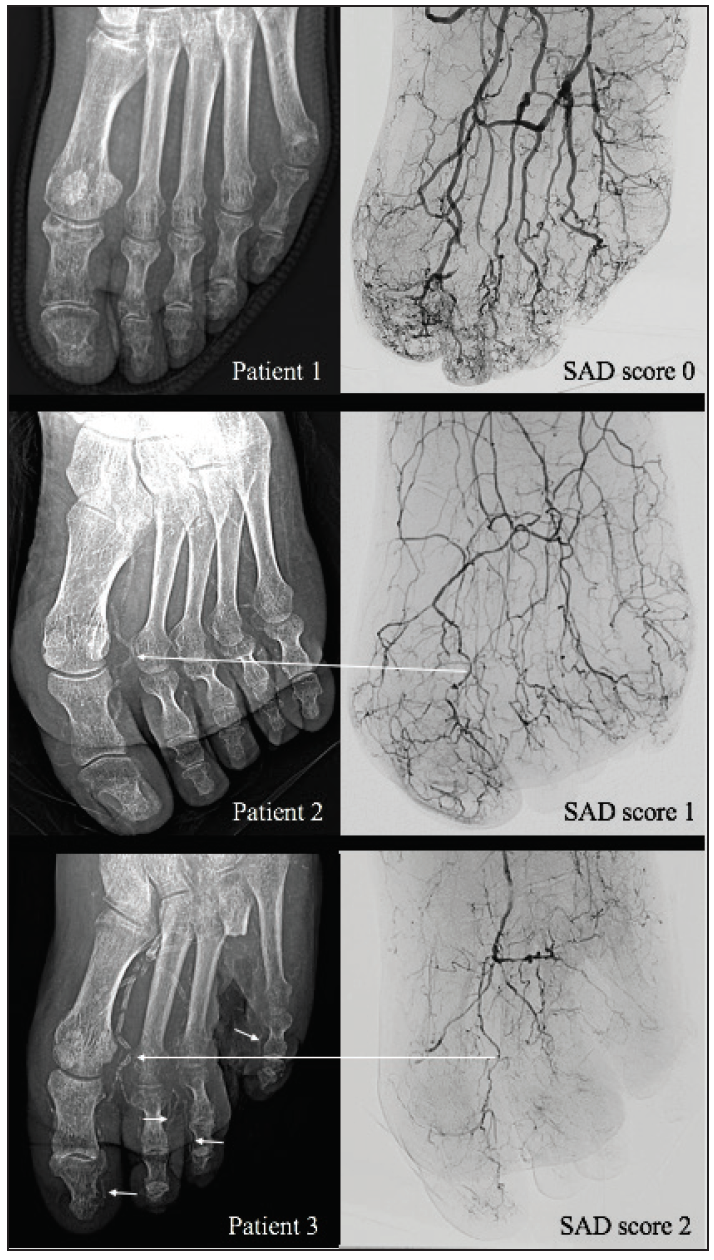
A true no-option CLTI patient can be defined as a patient without any residual vessels in the foot that could be a target for distal bypass or angioplasty. Some patients develop this condition after embolization or failed repeat revascularization attempts; however, most no-option CLTI patients today are affected by small artery disease (SAD). SAD is responsible for progressive failure of the foot distribution system, leading to a “desert foot” in the final stage. In Figure 2, we present a 3-level SAD score based on visual estimation of the angiographic imaging.2 SAD is strongly associated with medial artery calcification (MAC),3 which appears as a typical rail-track pattern of calcium, spreading in the entire vascular tree. We proposed a new 3-level MAC score based on plain foot x-ray (which demonstrated a powerful sensitivity and specificity in detecting for SAD), identifying SAD-MAC as a key player in CLTI.4 SAD-MAC scores were highly predictive of the patient’s fate in terms of healing, limb salvage, survival, and freedom from reintervention. Surprisingly, 45% of our patients presented with severe SAD-MAC scores, representing a no-option CLTI cohort in whom traditional approaches have a high failure rate.4
{kind=link}
Figure 2. Left column: x-rays of the anteroposterior forefoot in three patients with CLTI. Right column: anteroposterior forefoot angiography of the same patients. SAD score was categorized as: 0, absence of disease; 1, moderate (diffuse disease with narrow but patent arch, metatarsal, and digital arteries); or 2, severe (occlusion or extreme poverty of arch, metatarsal, and digital arteries). In patients 2 and 3, long arrows show the first metatarsal artery still open but completely calcified. In patient 3, short arrows show the extension of MAC into the occluded digital arteries.
IS pDVA TECHNICALLY FEASIBLE?
Inflow and outflow must be carefully evaluated before the procedure. Proximally, at least one below-the-knee (BTK) vessel must be open (with or without previous angioplasty and/or stenting) to function as the inflow of the arterialization. The target inflow artery at the crossover point must be treatable with a 3.5- to 4-mm stent. Patients with a history of previous vein stripping, harvesting, or thrombosis must be excluded. Distally, there must be a good venous target in the plantar vein system that is able to become the new foot distribution system. Preprocedural ultrasound is useful for evaluating the pedal veins.
What has been your own early experience with venous arterialization? What interested you in the LimFlow procedure, and how did you get involved in the study?
Dr. Kum: I was inspired to perform surgical deep venous arterialization (DVA) after listening to an enlightening talk by Professor Pramook Mutirangura from Thailand at VEITH 2010. I performed my first surgical case in 2012 on a patient with no-option CLTI. With the experience gained, I performed my first pDVA in Singapore in September 2013 with Dr. Schmidt. In July 2014 in Singapore, we performed the first of seven pDVAs in the LimFlow first-in-human trial.
Since then, we have learned from the experiences of many DVA advocates, including Drs. Pramook Mutirangura, Tadahiro Sasajima, Frank Veith, and Roberto Ferraresi, many of whom continue to offer ideas and words of encouragement. Together with the experiences in Europe and the United States, we continue to improve our patient selection, refine our technique, and improve our protocol for postprocedural care.
Dr. Schmidt: Immediately after the LimFlow procedure was introduced to our institution, we were excited to have a technique available for patients with absolutely no options for preventing major amputation. Dr. Kum, with whom we had already shared several other projects, introduced us and involved us with this procedure. The idea of performing this relatively old idea of DVA in a purely endovascular was very attractive. The anticipated advantages were the opportunity to avoid additional wounds at the foot level and, especially, the option to phlebographically examine the venous circulation and prepare the venous outflow in a more meticulous way by PTA and/or valvulotomy than with a purely surgical approach. We had to learn a lot in this new field.
In your experience to date, how would you describe the learning curve for the procedure, and what have you learned about it since your first case?
Dr. Schmidt: In most cases, the procedure is not too difficult to perform. Although this kind of endovascular treatment is a new experience for us, the learning curve is not long. Proctoring by someone experienced in the LimFlow procedure is extremely helpful. Approximately 5% to 10% of the cases appear to be challenging, mainly because of some unknown concomitant venous disease. In all cases, it is very important to understand the venous anatomy of the foot.
However, the most important phase of the treatment is the week- to month-long time span after the LimFLow procedure, when close monitoring for any changes in the patient’s clinical condition (swelling, pain, infection) and prompt adjustments to postprocedural care are essential to achieve a good long-term result. The postinterventional phase is when we are confronted with the longest learning curve, determining how best to eventually achieve limb salvage.
Dr. Kum: As with any new procedure, our first few cases were difficult. We had to deal with a complex group of patients, uncertain anatomy, and off-the-shelf devices that were not designed to perform the procedure. Since then, we have learned so much more about patient selection, including lessons on the location of crossing and the size of crossing stents to avoid any excessive steal syndrome from existing collaterals.
Valuable lessons on how to treat valves in the outflow with a valvulotome have also been learned. The “focalization” of blood with adjunct procedures to improve venous pressurization is an evolving concept. There is also a difference between treating a patient with no option for further revascularization where DVA is proposed to help (ie, no-option CLTI) versus a patient with a hopeless leg and extensive tissue loss such that any attempt at limb salvage would be futile. Also, the procedural steps have now been refined with the aid of a dedicated device (LimFlow), so we can now safely and predictably perform the procedure within 2 hours, from puncture to closure.
We have also learned a lot about postprocedural care, specifically wound care. DVA often requires 4 to 6 weeks before we see wounds granulate and transcutaneous oxygen pressure (TcPO2) rise. Ancillary procedures to manage patency and flow have been necessary to enable maturation of the arterialized circuit.
How would you describe the patient population included in the ALPS registry?
Dr. Kum: ALPS is a multicenter registry of 32 consecutive patients with no-option CLTI who were treated with the LimFlow procedure. These patients were pooled from dedicated centers with multidisciplinary teams from Alkmaar, the Netherlands; Leipzig, Germany; Paris, France; and Singapore. This is the largest cohort of consecutive LimFlow patients with follow-up to 2 years. It was a real-world cohort, with two-thirds of patients with diabetes, 100% with tissue loss, 71.9% with Rutherford 5 classification, and 28.1% with Rutherford 6 classification. In addition, 25% were on immunosuppression and 16% had dialysis-dependent renal failure. As many as 87.5% had a previous failed attempt at conventional intervention. Patients were deemed by the centers to have no further option for distal bypass or intervention; hence, they were at a high risk of major amputation. Outcomes were observed out to 2 years.
Dr. Schmidt: In our center, this treatment is reserved for desperate cases when no surgical option exists and at least one endovascular treatment has already been attempted. Usually, these patients are Rutherford 6 or rapidly progressive Rutherford 5. We have to be careful not to perform the LimFlow procedure too late, such as when infection or gangrene have progressed too far, because a prosthetic graft implanted close to the wounds or forefoot veins can thrombose during ischemia progression. Therefore, after seeing positive results in patients with very progressed CLTI, we now consider DVA earlier during the progression of critical ischemia.
What are the challenges of designing and conducting a study for a novel therapy for a challenging patient population such as this?
Dr. Schmidt: The main challenge for a study to prove the benefit for these challenging scenarios is the lack of a control group. Because these are patients where we find our backs against the wall, a randomized trial would be difficult to design. If we offer no treatment, many of them will inadvertently suffer from major amputation. It is difficult to set a benchmark for limb salvage with this procedure. If the natural course in these desperate cases ends in a major amputation rate of 50% to 75%, a limb salvage rate of 60% or more may indicate significant success.
Another challenge is to firmly tether the patient to the center where the procedure took place and where every major decision during the postinterventional phase is made in a team approach. Admission to health care professionals who are not experienced in this treatment may lead to wrong decisions and, eventually, unnecessary amputation.
Dr. Kum: Clinical trials for devices in this setting (eg, drug-eluting stents/balloons) for CLTI are difficult due to the complex nature of the patient and disease. Traditional endpoints like patency, target lesion revascularization, and amputation-free survival are well established. However, equally important endpoints such as complete wound healing add a different paradigm to clinical trials, and they are increasingly looked at to determine the efficacy of a device to address a pertinent clinical question. The effectiveness of an endovascular device is now evaluated by an outcome not entirely specific to the procedure, which can be challenging due to variable standards of wound care but is of huge importance to the welfare of the patient.
This is an important study in a CLTI cohort in which the definition and natural history of a no-option CLTI patient is poorly understood.
How do you define procedural and longer-term success for these difficult clinical presentations?
Dr. Schmidt: Procedural success is defined as achieving straight flow from the artery connected to the vein into the venous foot loop at the metatarsal level. However, in very few cases, we have also achieved clinical success with connecting more proximal tarsal veins to the arterial circulation in case of an occluded venous forefoot. Often, digital veins are not supplied retrogradely via the arterialized veins—at least not immediately postprocedure—due to their still-competent vein valves.
Long-term success is assessed clinically. The first weeks after the procedure are critical. Toes may become gangrenous, and minor amputations may be necessary. Whether long-term patency of the grafts to the venous foot circulation is important is currently unknown. However, close surveillance is necessary, and if reocclusion occurs before a clinically stable situation is achieved, reintervention should be performed. Our impression is that when healing has been achieved, the clinical situation remains stable—and the ALPS data confirm this. Potentially, some remodeling could be induced by the LimFlow procedure, preventing any ischemic deterioration in the long term.
Dr. Kum: Procedural success is typically defined as a patient who had a procedure that was considered a technical success, survived at least 30 days, and does not have an above-ankle amputation or clinically driven major reintervention. Long-term success for these patients is observed in wound healing, maintenance of ambulation, and pain reduction. Complete wound healing can be hugely impactful for these patients and demonstrates the impact of the therapy in a patient population headed for major amputation. The long-term follow-up from the ALPS study is encouraging in this respect.
What are the key highlights from the data gathered in ALPS?
Dr. Schmidt: The most important message of the ALPS registry is the impressive 79.8% limb salvage rate, which was achieved out to two years in patients of whom 78.1% were deemed to be at high risk for major amputation, according to the Society for Vascular Surgery’s Wound, Ischemia, and foot Infection (WIfI) classification. This was not only achieved at one highly experienced center but in a multicenter approach.
Another impressive finding was that a majority of patients healed their wound within 12 months. This rate and the time to wound healing compare well to existing CLI studies after arterial surgical or endovascular reconstruction.
Dr. Kum: The study has just been published in the Journal of Endovascular Therapy,1 and the results show that:
- Technical success was achieved in 97% of patients.
- Amputation-free survival was 83.9%, 71.0%, and 67.2% at 6, 12, and 24 months, respectively.
- Limb salvage was 86.8%, 79.8%, and 79.8% at 6, 12, and 24 months, respectively.
- Complete wound healing was achieved with 36.6%, 68.2%, and 72.7% of patients at 6, 12, and 24 months, respectively.
- In a period of 2 years, 142 TcPO2 measurements were performed. The median TcPO2 was 11 mm Hg preprocedure and 57.5 mm Hg 2 years postprocedure. The rise in TcPO2 measurements was statistically significant after 45 days.
What are your take-home messages from the ALPS registry experience?
Dr. Schmidt: The learnings from this initial experience have been very important, especially in optimizing postprocedural care in the first weeks. The long-term outcomes from the ALPS registry give increased confidence to proceed with the pDVA treatment in no-option patients.
Dr. Kum: There is now a new option for patients with no-option CLTI. Early experience of pDVA with the LimFlow device has shown the potential to resolve pain, heal wounds, and prevent major amputation, with durable results out to 2 years.
PATIENT PRESENTATION
This is the case of a 59-year-old woman with known PAD secondary to Churg-Strauss syndrome, now known as eosinophilic granulomatosis with polyangiitis. This rare condition causes inflammation of small- and medium-sized blood vessels. Her relevant comorbidities included type 1 diabetes mellitus, and she was an ex-smoker who quit many years ago.
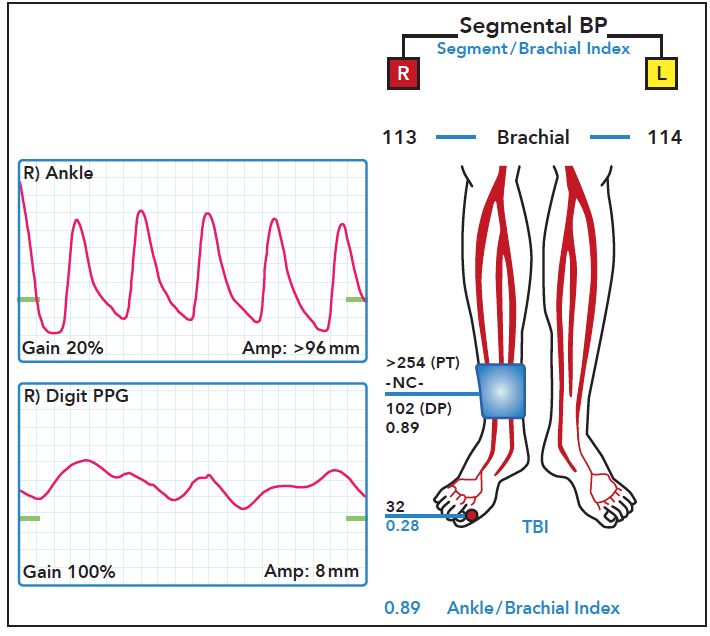
The patient presented in 2015 with left foot kissing ulcers and severe pain. She was considered for bypass using autologous vein, but no targets could be identified in the foot. She then underwent multiple attempts at endovascular revascularization, all of which failed. After undergoing a partial ray amputation followed by transmetatarsal amputation, she underwent a BTK amputation. She fared well until September 2017, when she presented with right lower extremity ulcers and pain involving D1 and D2 (Figure 1). Hemodynamic assessment at that time revealed a noncompressible ankle-brachial index (ABI), with a toe-brachial index (TBI) of 0.28, a toe pressure of 32 mm Hg, and flat digital waveforms (Figure 2).
{kind=link}
{kind=link}
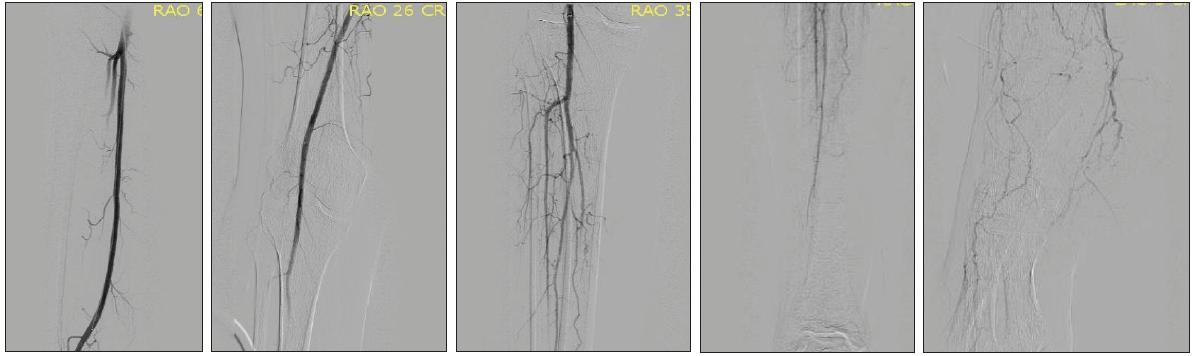
Given her history, she underwent full lower extremity angiography, which revealed severe distal tibial and foot disease (Figure 3). All treatment options were considered, including aggressive risk factor modification with aspirin and statins, arterial flow pump, and gentle wound care. Her other options were bypass and endovascular recanalization of distal tibial and pedal arteries.
{kind=link}
COURSE OF TREATMENT
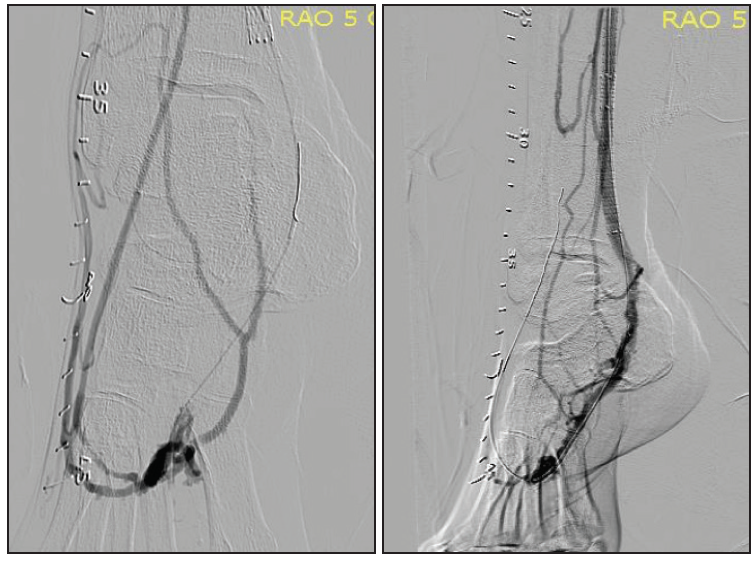
Bypass was not an option because there was no evidence of a distal foot target. Subsequently, two attempts at endovascular revascularization were made without success. Unfortunately, her ulcers and pain progressed over time. In February 2018, she was no longer tolerating her pain despite hydrocodone/acetaminophen, and the wound and erythema had worsened (Figure 4). At that point, an attempt was made to enroll her into the PROMISE I United States feasibility study, but she was excluded because of her vasculitis. This patient had no options except another BTK amputation. We reached out to LimFlow, Inc. and our hospital (University Hospitals Cleveland Medical Center) to consider a compassionate use of LimFlow to save this patient’s leg. After FDA and University Hospital Cleveland Medical Center authorized compassionate use, the patient underwent pDVA with the LimFlow system in April 2018 (Figure 5).
{kind=link}
{kind=link}
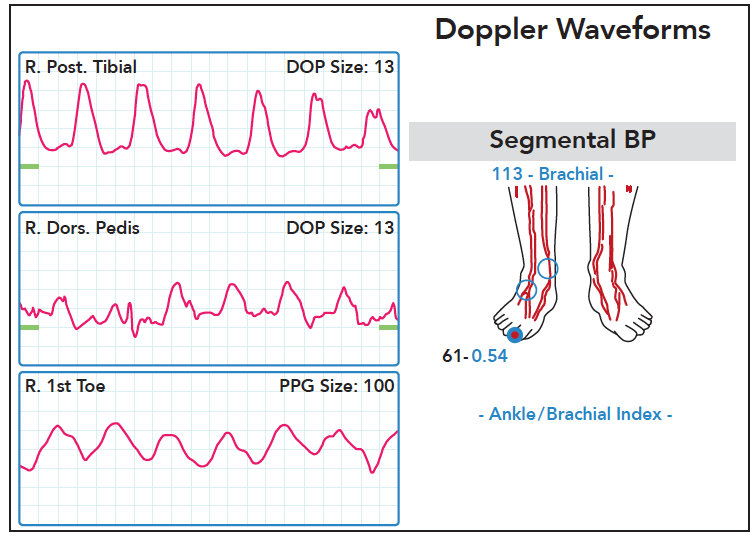
She had persistent pain for the first 2 to 3 weeks postprocedure, which was managed with analgesic medications. Gradually, she began to improve, and she underwent distal toe amputation of D1 and D2 approximately 4 weeks after the LimFlow procedure. By November 2018, her foot wound had completely healed (Figure 6). Despite total occlusion of the arterialized vessel at 7 months post–index procedure, her TBI had improved from 0.18 in April to 0.54 in November, with excellent waveforms (Figure 7).
{kind=link}
{kind=link}
DISCUSSION
Many of the challenges that patients with no options face are seen in this case. In 2015, this patient underwent BTK amputation after multiple procedures and months of pain. Similarly, in 2017, she underwent multiple procedures and care on her remaining limb without success, demonstrating the suffering and prolonged delay that patients with no option frequently encounter.
The case highlights how this procedure can have a significant impact and save limbs. For this patient, LimFlow prevented her from needing bilateral amputation. Keeping her leg improved her quality of life and emotionally and mentally reenergized her. I just saw her last month and she is doing fantastic, without a wound or any pain. With advanced therapies like LimFlow, we hope to save as many limbs as possible.