

- Home
- Companies
- Avery Biomedical Devices, Inc.
- Products
- Avery - Diaphragm Pacing System
Avery - Diaphragm Pacing System
The Avery Diaphragm Pacing System can provide ventilatory support for patients with chronic respiratory insufficiency whose diaphragm, lungs, and phrenic nerves have residual function. Typically, these patients have high spinal cord injuries, central sleep apnea or other central neurological disorders or a paralyzed diaphragm. A diaphragm pacing system consists of surgically implanted receivers and electrodes and an external transmitter with antennas worn directly over the implanted receivers. The external transmitter and antennas send radiofrequency energy to the implanted receivers just under the skin. The receivers then convert the radio waves into stimulating pulses. These pulses are then sent down the electrodes to the phrenic nerves, causing the diaphragms to contract. This contraction causes inhalation of air. When the pulses stop, the diaphragms relax and exhalation occurs. Repetition of this series of pulses produces a normal breathing pattern.
IMPROVES
Quality of life
Pacing is preferable to mechanical ventilation because it allows for normal breathing and speech patterns; eases eating and drinking; is small and operates silently; all of which improves the ability to actively participate in social and educational activities.
SAVES $20K/YR*
Over mechanical ventilation
A diaphragm pacing system generally costs less than $1,000 per year, and on average will pay for itself in 2 years, saving over $20,000 a year thereafter*.
REDUCES RISK
Of pneumonia & infections
Upper airway infections are less common due to the reduction in suctioning and elimination of external humidifier/ventilator circuits and tracheostomy tubes.
PROVIDES MORE
Freedom & independence
The Avery diaphragm pacer’s compact design, without bulky tubing and batteries, allows for greatly increased mobility and independence.
In March 1998, the U.S. Food and Drug Administration gave premarket approval (PMA) to the new Mark IV external transmitter for adult and pediatric patients who have lost neurological control of respiration. FDA premarket approval is required before Class III medical devices can be commercially distributed in the United States.
In advance of FDA approval, the Mark IV had been distributed in 24 countries worldwide. The Mark IV qualified for the CE Mark under the European Active Implantable Medical Device Directive in 1995.
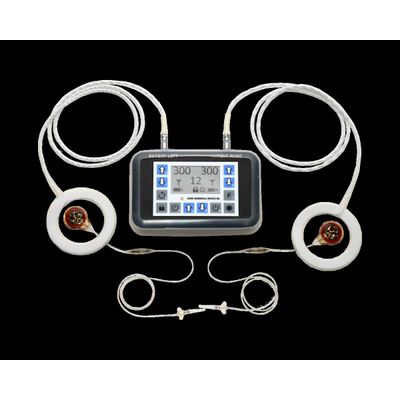
The Spirit Diaphragm Pacing Transmitter is CE Marked under the European Active Implantable Medical Device Directive as of 2017, and received full FDA Approval in November 2019. The transmitter is lightweight and features a backlight for nighttime viewing, clear graphic display, touch controls, and digital precision. For safety, it is also water resistant, has keypad locks, utilizes audible and visual alarms, and features bilateral redundancy.
The implanted receiver is a small electronic device, about the size of a US quarter and approximately 1/4″ thick, that receives radiofrequency energy and converts it to electrical impulses which stimulate the diaphragm.
The implanted electrode is a highly flexible stainless steel wire, insulated by silicone rubber, with a platinum nerve contact on one end, and a connector that mates with the receiver at the other.
The I-110 family of receivers were implemented for phrenic pacing in 1990 and approved by the US FDA in 1991.
An external antenna is worn over each implanted receiver and sends power and radio signals from the transmitter to the receiver transcutaneously. This radiofrequency coupled design means that there are no wires or plugs protruding from the skin, and no batteries in the implant that would require periodic replacement.
An antenna is a durable disposable item which requires periodic replacement. It is recommended that antennas be replaced prophylactically every six months. Antennas are available in one-meter and two-meter lengths.
Antennas do not contain latex. Additionally, no latex products are used in their manufacturing. Instructions for the use and care of antennas can be found here.
A surgical procedure is necessary to implant the electrode under the phrenic nerve and the receiver just under the surface of the skin. This procedure can be done cervically (via the neck) or thoracically (via the chest). For bilateral stimulation (stimulation of both phrenic nerves) two antennas, two electrodes and two receivers are needed. For unilateral stimulation (stimulation of only one phrenic nerve) one antenna, one electrode and one receiver are needed.
The procedure averages 2-4 hours in length, and the patient is typically discharged from the hospital 1-2 days later. Some procedures can be performed on an outpatient basis.
The decision as to which approach is appropriate is determined by the surgeon performing the procedure.
The thoracic approach involves a small (5-7 cm) incision made between a pair of ribs so that the phrenic nerve can be isolated alongside the heart. The surgeon places the electrode under or near the phrenic nerve and sutures it in place. The receiver is then placed just under the skin, usually from within the same incision.
The thoracic approach can be performed in a minimally invasive manner by using VATS (video-assisted thoracic surgery) techniques. Since a small camera is used to provide visualization of the operative site, the incision can be significantly smaller.
The thoracic approach can also be performed thoracoscopically and involves the use of multiple small (5-10 mm) incisions instead of one primary incision. Through these incisions, a camera and specially designed instruments are used to visualize the nerve and place the electrode. Thoracoscopic procedures can be performed with standard endoscopic instruments or by use of a surgical robot.
This approach is commonly chosen for the youngest pediatric patients since the anatomy of the neck is not sufficiently developed in these cases. It is also a common approach for patients who are suspected of having nerve damage so that the stimulation can occur below the presumed injury.
The cervical approach is also considered minimally invasive since it does not require a thoracotomy, or chest procedure.
It uses a small (3-5 cm) incision made in the area where the neck meets the torso. The phrenic nerve is isolated where it is most superficial, the scalenus anticus muscle. The surgeon places the electrode under the phrenic nerve and sutures it in place.
The receiver is then placed just under the skin, usually within a small pocket made on the upper part of the chest.
This approach is commonly chosen for older pediatric patients and adult patients who are known to have good phrenic nerve conduction. In addition to avoiding a thoracotomy, this approach has the advantage that it can be performed on an outpatient basis for some patients.
The primary purpose of intraoperative testing is to confirm stimulation of the phrenic nerve. Intraoperatively, diaphragm function can be confirmed via a number of methods including: visual observation of chest wall, palpation of the costal margin, observation of CO2 changes as measured by anesthesia equipment, and rarely, fluoroscopy.
The primary purpose of intraoperative testing is to confirm stimulation of the phrenic nerve. Additionally, preliminary threshold and amplitude settings can be assessed. These numbers can provide a baseline from which pacing can be established once healing is complete.
The thoracoscopic surgical technique is unique in that the camera allows for direct visualization of the diaphragm while under stimulation.
Breathing pacemakers have been implanted in hundreds of hospitals in over forty countries around the world. Upon request, ABD may be able to provide a referral to an experienced surgeon depending on the patient’s age, diagnosis, and geographical location.
Detailed instructions on the cervical and thoracic approaches are provided in the Instruction Manual. The thoracoscopic approaches and nerve grafting techniques are discussed in a number of peer-reviewed journal articles. An information packet — containing a manual and reprints of these articles — may be obtained by filling out an information request.
Pacing has many advantages over PPV, including : Breathing pacemakers provide respiratory function superior to mechanical ventilators since the inhaled air is drawn into the lungs by the diaphragm under negative pressure, rather than being forced into the chest under positive pressure. This is physiologically more accurate and comfortable for the patient.
Pacing patients are at much lower risk of upper airway infections including ventilator-associated pneumonia (VAP) due to the reduction in suctioning, elimination of external humidifier and ventilator circuits, and the potential removal of the tracheostomy tube in appropriate patients.
Most patients strongly prefer pacing over mechanical ventilation for a variety of reasons such as normal breathing and speech patterns, ease of eating and drinking and improved sense of smell.
Breathing pacemakers generally cost less than $1,000 per year in disposable supplies (antennas, batteries, etc.) to operate, which is substantially less than the rental fees and disposable supplies associated with a mechanical ventilator. On average, a diaphragm pacing system will pay for itself in roughly two years and save over $20,000 per year thereafter.
While all methods to pace the diaphragm share certain similarities, the Avery Diaphragm Pacing System System is the only device with full premarket approval from the FDA. Additionally, it has several distinct advantages, including : Breathing pacemakers use small implanted radiofrequency receivers to receive breathing pattern signals across the patient’s intact skin. Other systems use percutaneous electrode wires that pass directly through the skin that are at constant risk for infection and present ongoing wound care management issues. Additionally, such wires provide an electrical conduction path from outside to inside the body. Accidental contact between a percutaneous lead and other conductive elements could cause tissue damage or other injury.
The implanted electrodes use a compact, single contact design which stimulates the entire phrenic nerve at once, rather than multiple contact designs which can be surgically difficult to place and are subject to additional potential failure points. Because of this design, Avery diaphragm pacing systems can be implanted using a variety of minimally-invasive surgical approaches including cervical and thoracoscopic techniques.
For certain patients, the procedures can even be performed on an outpatient basis. For others, diaphragm pacing systems can be used in conjunction with intercostal or spinal accessory nerve grafting to restore diaphragm enervation and allow pacing in patients who otherwise would not be candidates.
The surgeon does not need specialized training in order to implant an Avery system, and no specialized equipment is required. Onsite technical assistance is provided at each surgery at no additional cost.
Avery diaphragm pacing systems are designed with bilateral redundancy for superior safety. Each diaphragm is paced by its own receiver, electrode, and external transmitter output. This independence provides an extra margin of safety as there is no single failure point which could cause the entire system to stop working. These devices have also been subject to rigorous environmental and electromagnetic testing by independent laboratories to ensure safety and efficacy.
Unlike other systems, the Avery transmitter is entirely self-contained and does not require a complicated external programmer to configure it. End user controls allow patients and their caregivers the flexibility to adjust the system as needed. They also use standard alkaline batteries which are readily available worldwide.
Avery diaphragm pacing systems are not contraindicated for patients with cardiac pacemakers or other implanted medical devices.
Avery has been commercially distributing diaphragm pacing systems since the early 1970’s. Since then, nearly 2000 patients have been implanted in over 40 countries establishing an unsurpassed record of safety and reliability.
Dependent on the patient’s age and geographic location, Avery can provide a referral to an experienced center.